

































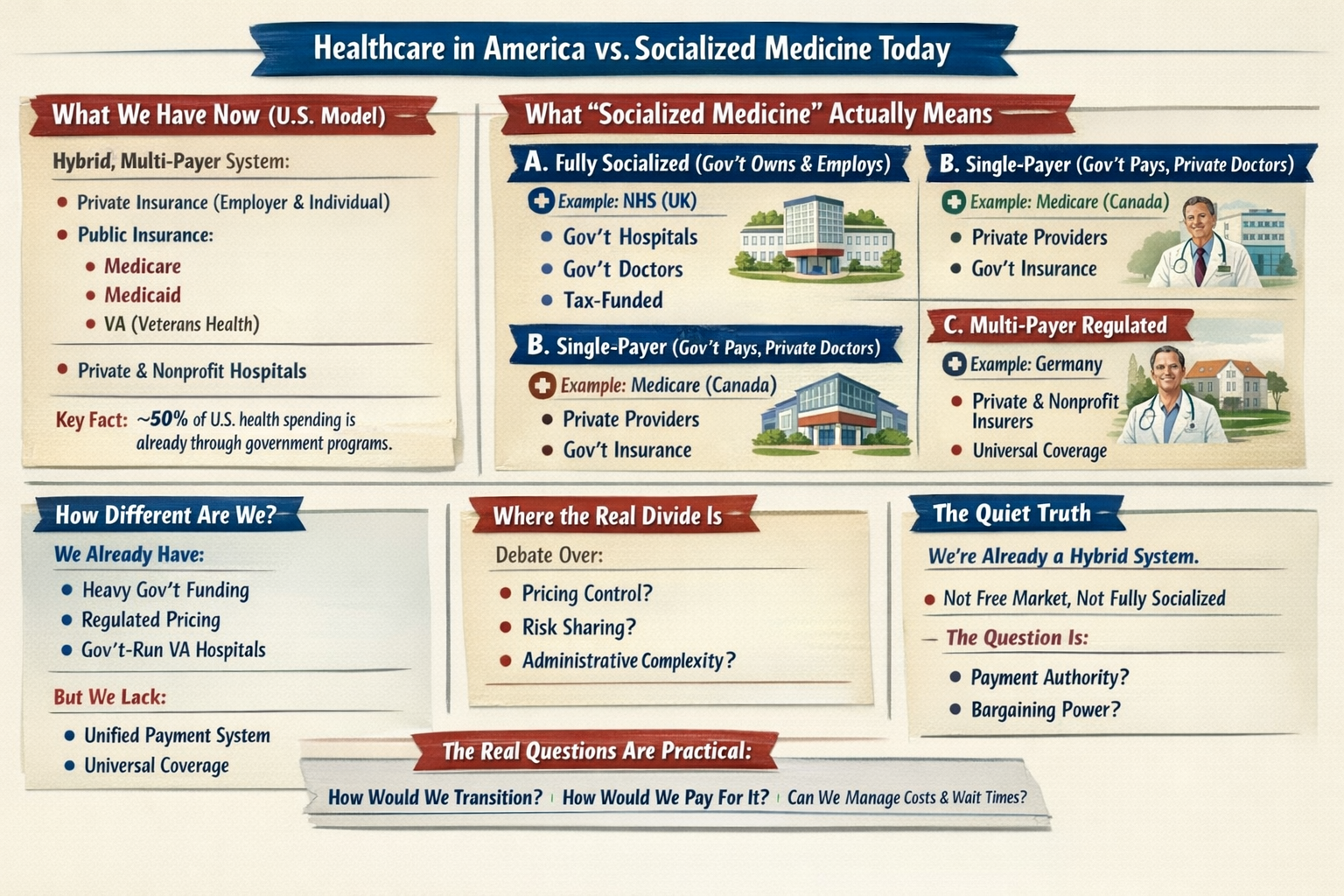
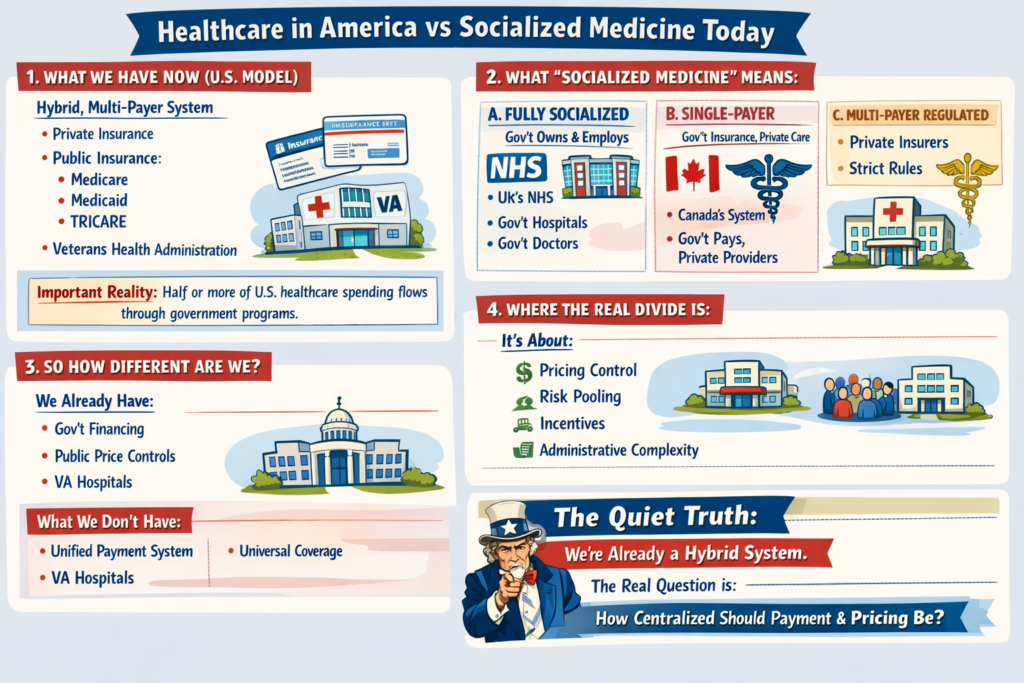
Healthcare in America vs Socialized Medicine Today
1. What We Have Now (U.S. Model)
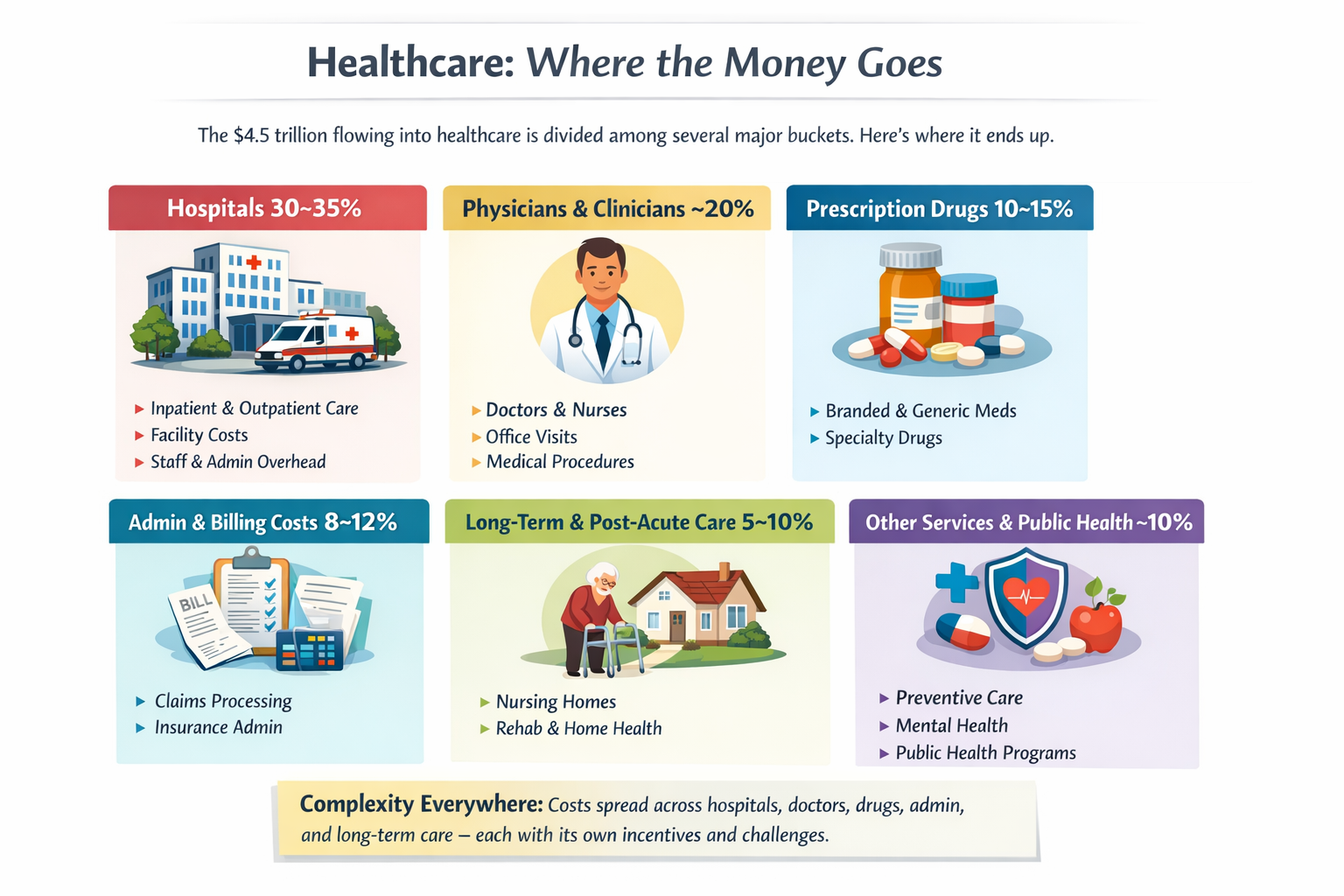
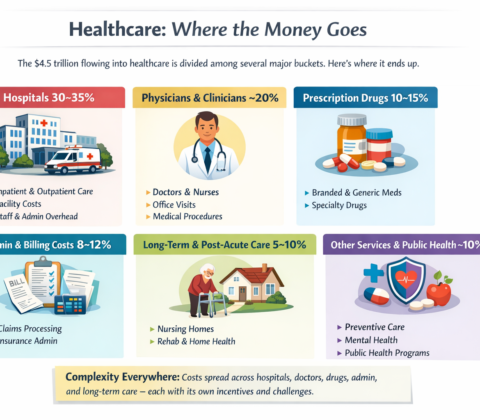
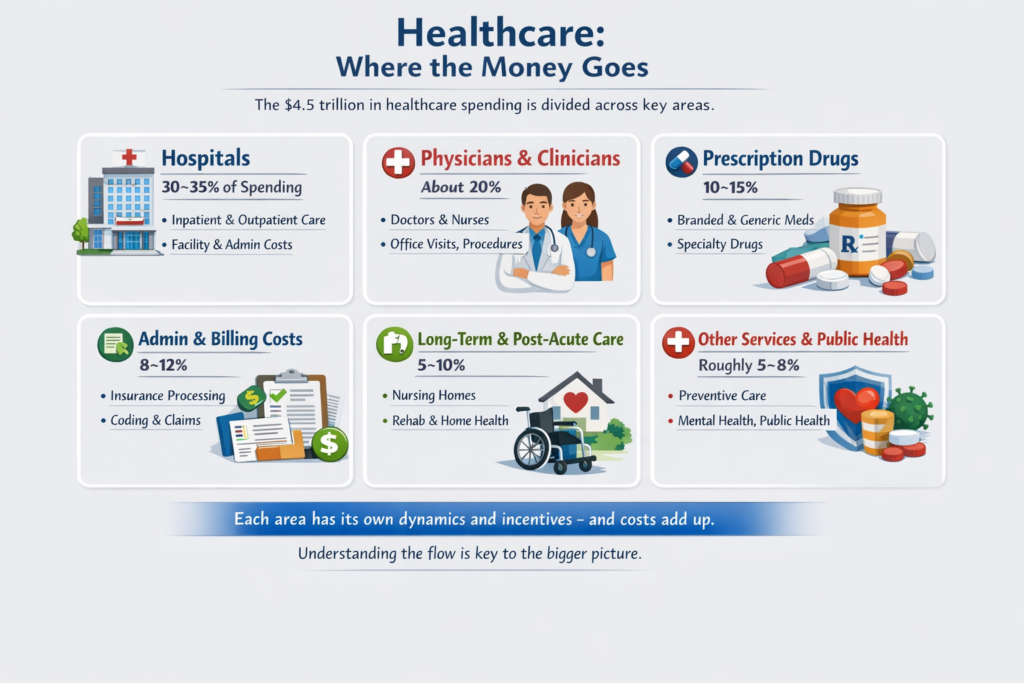
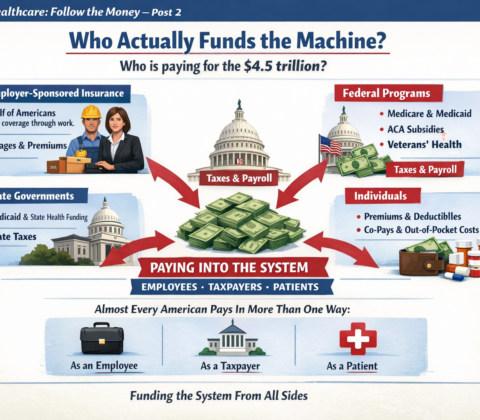
The U.S. system is a hybrid, multi-payer system:
-
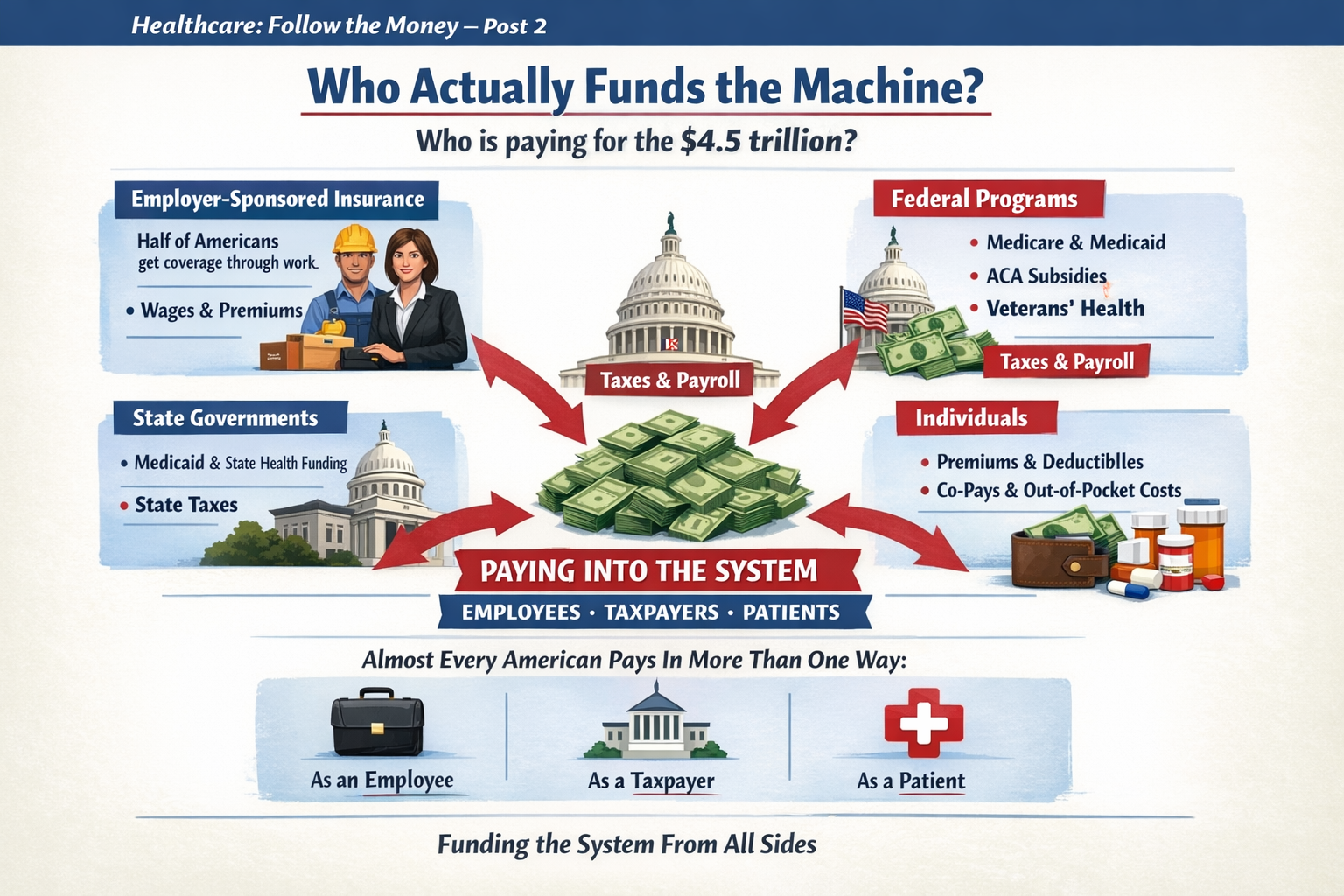
Private insurance (employer-based and individual market)
-
Public insurance:
-
Medicare
-
Medicaid
-
TRICARE
-
Veterans Health Administration
-
-
Private hospitals (mostly nonprofit, some for-profit)
-
Private physician practices (increasingly consolidated)
Important reality:
Roughly half or more of U.S. healthcare spending already flows through government programs. We are not a pure market system. We are a complex blend.
2. What “Socialized Medicine” Actually Means
People often use “socialized” loosely. There are actually three different models internationally:
A. Fully Socialized (Government Owns & Employs)
Example: National Health Service in the UK
-
Government owns hospitals
-
Doctors are government employees
-
Government sets budgets directly
-
Care funded through taxes
That’s true “socialized medicine.”
B. Single-Payer (Government Pays, Private Providers Deliver)
Example: Medicare (Canada’s system)
-
Private hospitals & doctors
-
Government is the main insurer
-
One public payment system
-
Funded via taxes
This is not government-run hospitals — it’s government-run insurance.
C. Multi-Payer Regulated System
Example: Statutory Health Insurance
-
Private and nonprofit insurers
-
Strict national rules
-
Price controls
-
Universal coverage mandate
3. So How Different Are We?
Structurally:
-
We already have heavy government financing.
-
We already regulate pricing in public programs.
-
We already operate large government-run care systems (VA hospitals).
-
We already subsidize private insurance through tax exclusions.
What we don’t have:
-
A unified payment structure
-
National price controls across the board
-
Universal automatic coverage
-
Simplified billing
The biggest structural difference isn’t just “who pays.”
It’s:
-
Fragmentation
-
Administrative layering
-
Pricing freedom in private markets
-
Employment-tied insurance
4. Where the Real Divide Is
The debate isn’t simply:
Private vs Socialized.
It’s about:
-
Who controls pricing?
-
How risk is pooled?
-
How incentives are aligned?
-
How much administrative complexity is tolerated?
Even a “socialized” system still rations care — just differently (wait times vs cost-sharing).
Even our current system has price controls — just unevenly applied.
5. If the U.S. “Moved Toward Socialized” — What Would Actually Change?
Not necessarily hospital ownership.
More likely changes would include:
-
Centralized bargaining power
-
Uniform reimbursement rates
-
Elimination of employer-based insurance
-
Tax-based funding instead of premium-based funding
-
Dramatically reduced administrative overhead
-
Reduced insurer role
The money flow changes.
The power centers shift.
Administrative structure simplifies.
But doctors would still practice medicine.
Hospitals would still exist.
Care would still be rationed — just through different mechanisms.
6. The Quiet Truth
We are already halfway between models.
The U.S. system is not a free market.
It is not socialized.
It is a layered hybrid with competing incentives.
The question isn’t:
“Would we become socialized?”
The real question is:
“How centralized do we want payment and pricing authority to be?”
That’s a structural debate — not just a funding debate.
To go deeper, we have to explore:
-
What would actually happen to costs?
-
What happens to innovation?
-
What happens to wait times?
-
Or what a realistic transition would look like?
The real questions aren’t ideological. They’re mechanical:










































































































































































































The Electoral College: A Solution Looking for the Right Problem? – Video
Most debates about the Electoral College start with people choosing sides. One side wants to keep it. The other wants to abolish it.
I think the more interesting question is: What problem was it designed to solve, and does that problem still exist?
In 1787, information traveled at the speed of a horse. Most citizens knew little about candidates from distant states. The United States was less a single nation than a collection of states agreeing to work together. The Electoral College was part compromise, part practical necessity, and part protection against direct democracy in a world where voters had limited information.
For its time, the system made sense.
Today, none of those conditions exist.
——————————–
A constitutional convention to redesign the whole thing?
I don’t know.
What I do know is that every system solves one problem by creating another.
A pure popular vote values every vote equally, but raises concerns about population concentration.
The Electoral College protects state influence, but leaves many voters feeling irrelevant.
Winner-take-all states simplify elections, but turn most states into spectators.
There may not be a perfect answer. There may only be better compromises.
Before we argue about which system to adopt, we should at least agree on which problem we’re trying to solve.
If we can’t answer that question, we’re just rearranging the furniture.
And unlike the spare toilet paper at my house, nobody seems to know where the solution is stored.
The Electoral College asks how states should be represented.
Ranked-choice voting asks how voters should be represented.
Maybe before we decide which system is best, we should decide whose voice we are trying to hear more clearly.
Share this:
Like this: