Skip to content

We see the tents.
We volunteer.
Not charity. Not awareness campaigns. Not temporary fixes.
Capital, invested with intent
Someone rallies a community.
Railroads weren’t built by committees waiting for permits.
Not awareness.


It’s under overpasses.
Cities clear areas and call it progress.
Address what’s immediately visible.
A system that moves slowly.
Not compassion.
Nothing connects.
Not:
But:






In apartments.
Homelessness over here.
Pieces that exist.
Less visible.
If the pieces are already there…




Posts in Category: Mental Healthcare
When Seeing Isn’t Enough, Who Builds?
 When Seeing Isn’t Enough, Who Builds?
When Seeing Isn’t Enough, Who Builds?
We’ve become good at noticing problems.
We see the tents.
We see the people fading away.
We see the cracks in systems that were supposed to catch them.
And we often respond.
We volunteer.
We donate.
We organize what little we can.
But noticing isn’t the same as building.
The real gap is in the people and organizations who actually structure solutions.
Not charity. Not awareness campaigns. Not temporary fixes.
I mean the kind of work that requires:
Capital, invested with intent
Teams, operating with accountability
Systems, designed to scale
Without that, even the best efforts stay islands.
There are occasional sparks.
Someone rallies a community.
A small operation starts and grows.
News catches it because it’s novel, or outrage makes it visible.
But those sparks are rare. And rare sparks can’t hold a fire.
We’ve trained ourselves to believe that scale only comes from government, or from huge organizations.
But history shows otherwise.
Railroads weren’t built by committees waiting for permits.
Cities weren’t lit by ideas held back by bureaucracy.
Movements weren’t started by people waiting for permission.
Scale comes when someone decides to start building—and then invites others to join.
That’s the space we’re missing now.
Not awareness.
Not compassion.
Not even outrage.
We’re missing builders.
People willing to put together the teams, the capital, the structure, and the commitment to make solutions grow.
We may not know the full answer.
No single person does.
But the signal is clear: wherever there’s a problem too big for charity and too complex for government… there is a role for builders.
Somebody has to start.
Share this:

We See It Every Day. So Why Isn’t Anything Changing?

We See It Every Day. So Why Isn’t Anything Changing?
You don’t have to go looking for it anymore.
It’s under overpasses.
Along sidewalks.
In places that used to feel like part of the normal rhythm of a city.
Tents. Makeshift shelters. People existing in plain sight, but somehow outside of everything around them.
We see it enough now that it’s become background.
And when something becomes background, it stops demanding answers.
There are responses, of course.
Cities clear areas and call it progress.
Organizations step in where they can.
Churches open kitchens, shelters rotate beds, volunteers show up with good intentions.
None of it is wrong.
But none of it is changing the direction of the problem.
We’ve settled into a pattern:
Address what’s immediately visible.
Move it. Manage it. Contain it.
Then repeat.
Over and over.
There’s also an assumption sitting underneath all of this:
That if the problem is big enough, government will eventually organize around it.
But this isn’t something that fits cleanly into a single department, a single budget, or a single political cycle.
So it gets divided, delayed, and debated.
And while that happens, the visible part keeps growing.
On the other side, there’s charity.
And there is a lot of it.
People care. They show up. They give time, food, money.
But most of it exists in small, isolated pockets.
A meal here. A bed for the night. A temporary service.
It helps—but it doesn’t carry forward.
It resets every day.
So we end up in between two things that aren’t built to solve it:
A system that moves slowly.
And efforts that don’t scale.
That leaves something missing.
Not compassion.
Not awareness.
Something more basic than that.
Nothing we’re doing is designed to grow into a solution.
Nothing connects.
Nothing compounds.
Nothing builds on itself.
And that’s the part that’s easy to miss, because everything we are doing looks like action.
It just doesn’t add up to progress.
At some point, the question changes.
Not:
Why is this happening?
But:
Why isn’t anything we’re doing capable of getting ahead of it?
Because those are two very different problems.
And only one of them can actually be built for.

Share this:

Making America Sick — Part 3 of 4: Why He’s Doing It? The Broken Compass
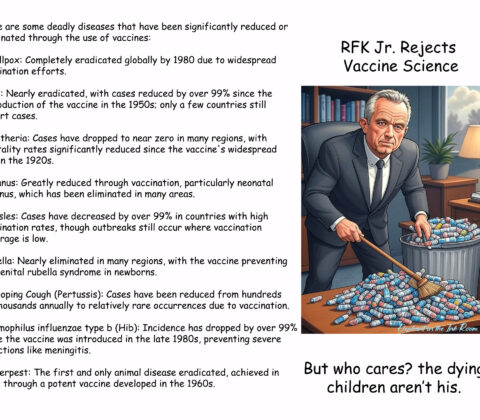
There is a question that stops most people when they look at the measles outbreaks, the whooping cough deaths, the hollowed out research institutions and the children who will go unvaccinated this fall because their parents received confusing guidance from the federal government. The question is simple and almost impossible to answer through a normal political lens.
How does he look at this and not stop?
It is the right question. And if you are looking for the answer in conventional political motivation — ambition, corruption, cynicism — you will not find it, or at least not find enough of it to explain what we are watching. Kennedy is not profiting directly from dismantling vaccine policy. He is not, by any reasonable measure, doing this for personal financial gain. He genuinely believes, as far as anyone can tell, that he is helping.
That is what makes him so dangerous.
To understand what is actually happening you have to set aside the political framework entirely and pick up a different one. Those who have spent careers working in mental health and addiction treatment will recognize the pattern immediately, not because Kennedy is simply an addict — recovery is real and people rebuild their lives completely — but because there is a specific kind of cognitive reorientation that prolonged substance use can produce in certain people, particularly those who were already wired toward intensity, pattern recognition, and distrust of authority. It does not announce itself. It does not look like impairment from the outside. It looks, in fact, like conviction.
Here is how it works. The brain’s threat assessment system, disrupted by years of substance use, can become permanently recalibrated. Not broken exactly — still functional, still capable of sophisticated reasoning — but reset to a baseline of suspicion that a normal risk environment cannot satisfy. Everything gets filtered through a framework that asks not “what does the evidence show” but “who benefits from me believing the evidence.” Once that filter is in place it is essentially self-sealing. Contradicting evidence doesn’t weaken the belief — it strengthens it, because contradiction becomes proof that the threat is real enough to require active suppression.
Kennedy wrote in a 2021 book that he rejected germ theory — one of the foundational principles of modern medicine, established over 150 years ago — in favor of miasma theory, the pre-scientific idea that disease arises from environmental corruption rather than specific pathogens. This is not a fringe position he stumbled into. He argued for it at length, in print, under his own name. And yet he continues to insist he is following the science. From inside that framework, he is. The science he trusts is the science that confirms what his recalibrated threat assessment already told him was true. Everything else is captured, corrupted, or bought.
This is not unique to Kennedy and it is not unique to addiction. It is a well-documented feature of how human cognition responds to prolonged trauma, chronic stress, and certain kinds of neurological disruption. What is unusual is the scale at which we are now watching it operate. Most people who develop this kind of framework do so in private, or in communities of like-minded believers, where the consequences are limited. Kennedy developed it in public, refined it over decades, built a following around it, and then traded that following for the most powerful public health position in the world.
The cruelest irony is that his instincts were not entirely wrong at the start. Corporate influence on research is real. The pharmaceutical industry has a documented history of suppressing inconvenient findings. Public health institutions did make serious errors during the pandemic that damaged trust. Kennedy’s original antenna was picking up genuine signals. But a broken compass that points slightly wrong will take you further and further from your destination the longer you follow it. By the time you are rejecting germ theory and redesigning the childhood vaccine schedule based on a country that provides universal free healthcare and has a population smaller than Texas, you are not where you started. You are somewhere that looks nothing like the riverbanks you once protected.
And the children getting measles in South Carolina cannot tell the difference between a broken compass and a working one. They just get sick.
What makes this particularly resistant to the normal corrective mechanisms of democratic accountability is that Kennedy speaks the language of his critics fluently. He knows what evidence-based medicine sounds like. He knows how to invoke transparency and scientific rigor and institutional accountability. He uses that language not to engage with the evidence but to reframe his rejection of it as a higher form of engagement. This is not stupidity. It is something more difficult to counter than stupidity, because you cannot simply show him the data. The data is part of the system he has already decided cannot be trusted.
Which brings us to the only thing that has ever worked against this kind of entrenchment — not argument, not outrage, not the correct facts delivered with sufficient force. What works is structure. Rules. Institutions with enough independence and enough legal authority to say no regardless of what any individual believes. Courts. Professional bodies. State governments. The accumulated weight of democratic process applied with enough consistency that no single broken compass can redirect the whole ship.
Those structures exist. They are fighting back. And that is where we are going next.

Share this:

Making America Sick — Part 2 of 4: The Damage
When Robert F. Kennedy Jr. took office in February 2025, the Department of Health and Human Services oversaw food and hospital inspections, health insurance for roughly half of the American population, vaccine recommendations, and the scientific research infrastructure that underpins most of what your doctor tells you. It was imperfect, often bureaucratic, and in genuine need of reform in places. What it did not need was to be systematically dismantled by someone who rejected the scientific foundations it was built on.
That is what happened anyway.
Within his first two months Kennedy announced the elimination of approximately 10,000 HHS jobs on top of another 10,000 employees who had already taken buyouts, collapsed 28 agencies into 15, and closed half of HHS’s regional offices. The cuts did not fall evenly. They targeted, as 19 state attorneys general would later document in federal court, specific programs and areas of expertise — the ones Kennedy had already decided were part of the problem. Infectious disease surveillance. Vaccine research. The scientific advisory infrastructure that had taken decades to build.
The research bleeding is quieter than the vaccine headlines but may prove more lasting. The National Institutes of Health cut approximately $2.7 billion in research funding, including a 31 percent reduction in cancer research. Five hundred million dollars in contracts to develop vaccines using mRNA technology, the same technology that saved millions of lives during the pandemic were canceled. Four NIH directors were fired or forced out. The FDA’s vaccine chief was removed. A CDC director Kennedy himself had hired was gone within a month. As one Georgetown University public health law professor put it, America is being hollowed out of its scientific leadership, and it will be extraordinarily difficult to reverse.
But it is the vaccine story that will be most immediately felt in pediatricians’ offices and school hallways across the country.
Kennedy promised during his confirmation hearings that he would not touch vaccine policy. Instead he fired all 17 sitting members of the CDC’s Advisory Committee on Immunization Practices, the expert body that has guided vaccine recommendations since 1964 and replaced them with known vaccine skeptics. The reconstituted committee promptly began downgrading recommendations. Then in January 2026, the CDC unilaterally reduced the universally recommended childhood vaccine schedule from 17 vaccines to 11, cutting protection against rotavirus, influenza, hepatitis A, hepatitis B and meningococcal disease from routine recommendations, not based on any new safety data, but modeled after Denmark, a country with universal free healthcare that is an outlier even among its European peers.
The consequences are not theoretical. A measles outbreak has spread to 26 states with over 960 confirmed cases centered in South Carolina. Two children have died from whooping cough. Vaccination rates have been falling since Kennedy took office. Last flu season saw 280 child deaths from influenza, the highest toll in more than a decade, and the federal government has now made the flu vaccine a matter of parental discretion rather than routine recommendation.
There is a clock ticking that most people don’t know about. Major health insurers pledged to keep covering the old vaccine schedule through the end of 2026. That pledge expires in December. After that, whether parents pay out of pocket for vaccines that were covered last year is an open question, and in a country where cost is already a barrier to preventive care for millions of families, the answer will show up in infection rates within a year or two.
None of this happened by accident. None of it happened without warning. Kennedy’s record as a vaccine skeptic was not hidden during his confirmation process, it was the central concern of every senator who questioned him, and he addressed each concern with a promise he did not keep. The damage being done to American public health is real, it is documented, and it is the direct result of placing ideological conviction above scientific evidence at the highest level of the public health system.
The question worth asking, and the one we will address next, is not whether Kennedy knows what he is doing. He does. The more useful question is why a genuinely intelligent person, with a real history of fighting for public health, arrived here. Because the answer to that question is the one that might actually help us understand how to stop it from happening again.
Share this:

Making America Sick — Part 1 of 4: The Man Who Knew Better
There is a version of Robert F. Kennedy Jr. that history should remember favorably.
As an environmental attorney in the 1980s and 90s, Kennedy was the real thing. He sued polluters, won, and made them pay. He fought corporations that dumped toxins into waterways serving poor communities who had no other advocate. He understood science, used it rigorously, and trusted it when it supported the case he was making, which it usually did, because the science on industrial pollution is not complicated. Corporations were poisoning people, Kennedy proved it, and he made them stop. That is not the biography of a crank. That is the biography of someone who understood exactly how institutions can be corrupted by money and power, and fought back effectively.
That understanding, that institutions lie when money is involved, is important. Because it wasn’t wrong. It was the seed of everything that came later, and like a lot of things that start from a kernel of truth, it eventually grew into something that consumed the original plant entirely.
Somewhere between the courtroom victories and the podcast appearances, Kennedy’s working theory shifted. Institutions sometimes lie became institutions always lie. Follow the money when evaluating a specific claim became follow the money as a substitute for evaluating evidence at all. The man who once used science as a sword against corporate corruption began using corporate corruption as a reason to reject science itself.
The drug years almost certainly played a role. Kennedy has spoken openly about his heroin addiction and recovery, and deserves credit for that honesty. But what he has never fully reckoned with publicly, and what anyone who has worked in addiction and mental health will recognize immediately, is that sustained substance use doesn’t just damage the body. It rewires the framework through which a person processes trust, authority, and risk. It can leave someone genuinely intelligent operating from a threat-assessment system that is permanently calibrated too high. Everything becomes suspect. Every institution becomes an enemy. Every simple answer becomes more trustworthy than a complex one, because complexity itself starts to feel like manipulation.
This is not a diagnosis. It is a pattern that professionals in mental health and addiction recognize, and it matters here because it explains something important: Kennedy is not stupid. He is not simply corrupt. He is a genuinely intelligent person operating from a framework that was damaged long before he ever set foot in the Department of Health and Human Services, and that framework is now being applied to the health of 330 million Americans.
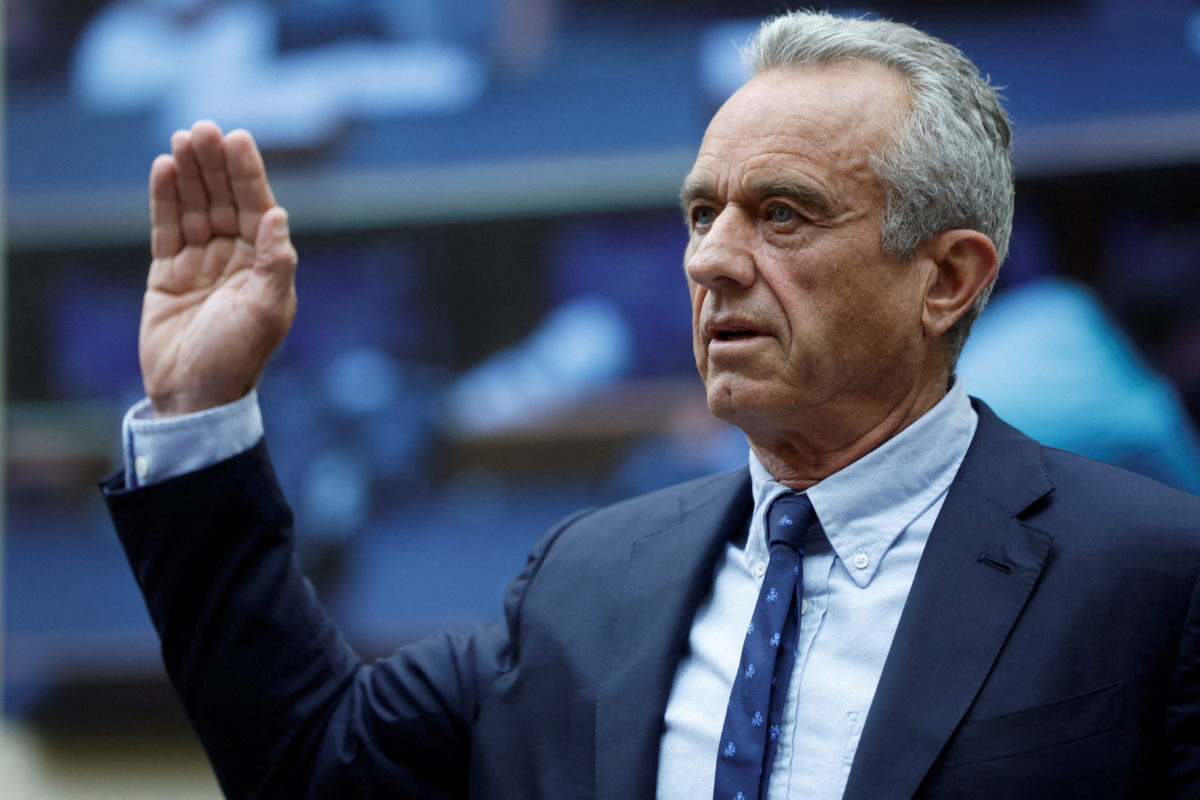
He was confirmed as Secretary of Health and Human Services in February 2025, after a Senate process in which he promised, repeatedly, that he would not dismantle vaccine policy, would not politicize public health, and would bring transparency and accountability to institutions that had lost public trust during the pandemic. Those were not unreasonable promises. Some of them were even things his critics could agree were worth doing.
He has broken nearly all of them.
What is less often discussed is how he got there. Kennedy’s path to confirmation ran directly through his decision to drop his independent presidential campaign and deliver his followers to Trump. The job was, by most credible accounts, the arrangement. Not a reward for expertise in public health. Not a record of administrative competence. A political transaction between two men who had spent years distrusting the same institutions, for very different reasons, and who each believed they were the one doing the using.

Share this:

A Text Message and FDA Approval – A COMPANION PIECE TO THE SERIES: MAKING AMERICA SICK — ROBERT F. KENNEDY JR.
When good things happen for the wrong reasons, and the wrong things happen anyway
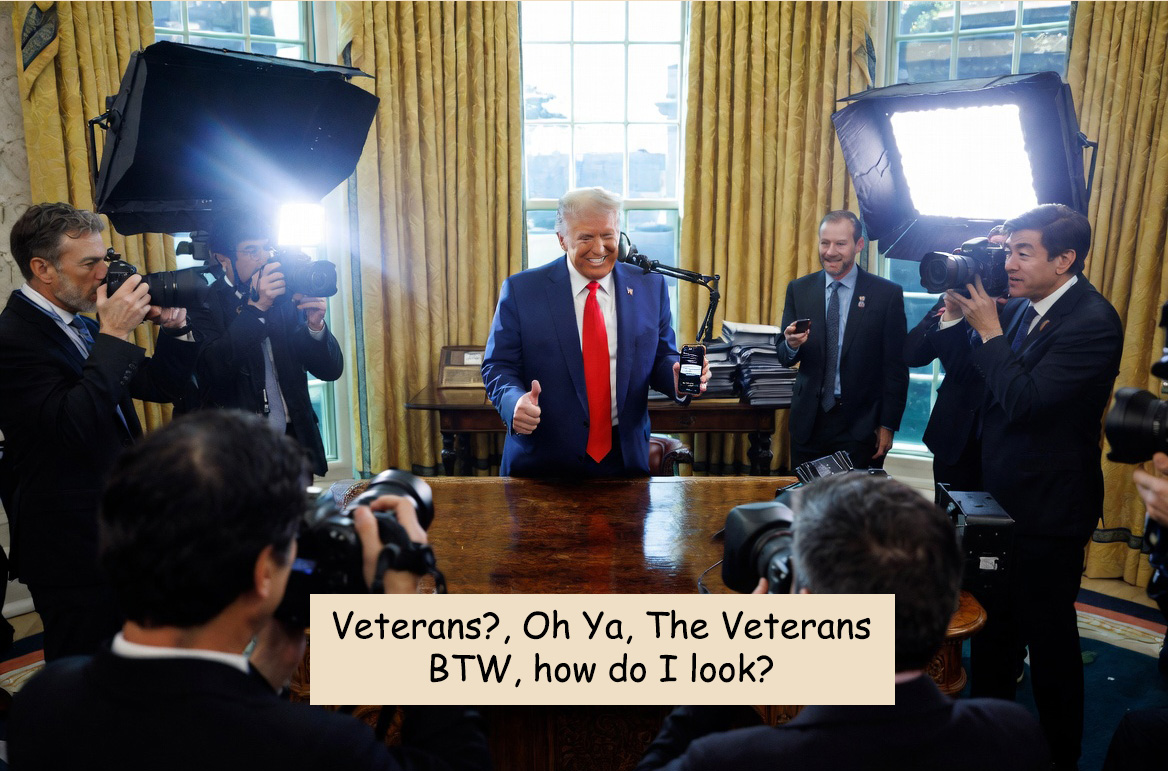
On Saturday, April 18, 2026, President Trump signed an executive order directing the FDA to fast-track its review of psychedelic drugs including ibogaine, psilocybin, and MDMA for the treatment of PTSD, depression, and traumatic brain injuries in military veterans. He stood in the Oval Office flanked by RFK Jr., Dr. Oz, podcaster Joe Rogan, and Marcus Luttrell, the decorated Navy SEAL whose story became the film Lone Survivor. It was, by any measure, a striking scene.
And here is the uncomfortable truth: the science behind this decision has genuine merit. A 2024 Stanford study found that veterans treated with ibogaine showed an 80 to 90 percent reduction in symptoms of depression and anxiety within a single month. For over twenty years, more than 6,000 veterans per year have died by suicide, a rate more than twice that of the civilian population. When people are dying at that scale, the calculus around acceptable risk changes. Sometimes you take the risk. Sometimes you throw the dice.
So credit where it is due: if this research is conducted properly, it could save lives. That matters. That is real.
“Sounds great. Do you want FDA approval? Let’s do it.” — President Trump, responding to a text from Joe Rogan
Policy by Text Message
But here is where the story gets complicated, and where the parallels to my ongoing series on Robert F. Kennedy Jr. become impossible to ignore.
This executive order, according to officials present, was written in less than a week. Its genesis was not a briefing from the VA, or a report from the National Institutes of Health, or years of advocacy from veterans’ organizations, though those voices exist and have been pushing for this research for years. Its genesis was a text message from Joe Rogan. Trump’s reply, as Rogan told it from the Oval Office: “Sounds great. Do you want FDA approval? Let’s do it.”
This is the same governing philosophy we see throughout this administration’s approach to public health. RFK Jr. didn’t dismantle vaccine confidence programs because of rigorous scientific review. He did it because of ideology, grievance, and the gravitational pull of a particular media universe. Trump didn’t fast-track psychedelic research because of a systematic review of veteran health outcomes. He did it because a podcaster texted him and it sounded good.
The mechanism is identical. The outcomes just happen to point in opposite directions.
The Hypocrisy the Headlines Won’t Tell You
While this announcement was being celebrated and it deserves some celebration the Department of Veterans Affairs has been quietly hemorrhaging the people who actually serve veterans every single day. Thousands of VA employees have been cut or are under threat as part of the administration’s broader federal workforce reductions. These are the people who answer phones, process disability claims, run mental health clinics, and sit across from veterans in crisis.
Ibogaine, even under an optimistic timeline, will not be widely available to veterans for years. The research still needs to be done properly. The cardiac risks, ibogaine has been linked to fatal heart arrhythmias and is connected to over thirty deaths in the medical literature — need to be understood and managed. The FDA approval process, even a fast-tracked one, takes time.
So what happens to the veteran who calls the VA crisis line next Tuesday and nobody answers? What happens to the veteran waiting eighteen months for a disability claim decision while staff positions sit empty? They don’t have Joe Rogan’s number. They don’t have a Lone Survivor story to tell in the Oval Office. They have a phone number and a waiting list.
This administration has demonstrated, repeatedly, that access to presidential attention and federal resources is mediated not by need, but by platform. By visibility. By whether you are useful to the political performance of the moment. Veterans, as a group, are enormously useful as symbols. As a bureaucratic constituency with daily, grinding needs they are less convenient.
The Thalidomide Shadow
Those of us old enough to remember thalidomide understand the cost of moving too fast. That drug approved in Europe, thankfully blocked in the US by one courageous FDA reviewer caused severe birth defects in thousands of children. The FDA’s deliberate pace exists for a reason. It was written in tragedy.
Ibogaine is not thalidomide. But it carries real risks, and the pressure now being applied to the FDA approve this in “weeks, not years” as the FDA commissioner suggested should make anyone who remembers that history uneasy. Speed driven by political momentum is not the same as speed driven by scientific confidence.
The research should proceed. The clinical trials should be funded. The veterans who have traveled to Mexico to access ibogaine treatments because they had no legal option at home deserve a legitimate pathway. All of that is true.
But “do you want FDA approval? Let’s do it” is not a drug approval process. It is a vibe. And we have seen, in this administration’s approach to public health writ large, what governing by vibe costs us.
Hold Both Truths
The hardest intellectual task in political commentary right now is holding two truths simultaneously when one of them gives comfort to people you disagree with. So let me be clear one final time: this research, done properly, could save veteran lives. That is good. That is worth fighting for regardless of who signs the order.
But the way it was done, by text message, in a week, surrounded by cameras and celebrities, while the VA workforce is being dismantled behind the scenes, is not a veterans policy. It is a veterans performance. And the veterans who will be waiting for ibogaine to navigate clinical trials and FDA approval while their local VA mental health clinic loses half its staff deserve to know the difference.
Good outcomes for bad reasons are still good outcomes. But they do not absolve the bad reasons. And they do not fill the staff positions that were cut last month.
This is a companion piece to the ongoing series Making America Sick: Robert F. Kennedy Jr., examining the Trump administration’s approach to public health, science, and the machinery of medical governance.
Published April 2026
Share this:

Robert F. Kennedy Jr – Making America Sick
Our next series will take on Robert F. Kennedy Jr and what he has done to America’s Health and Youth, and why, in the year he has been in Office.
This is a 4 part series.
Making America Sick — Part 1 of 4: The Man Who Knew Better
Making America Sick — Part 2 of 4: The Damage
Making America Sick — Part 3 of 4: Why He’s Doing It? The Broken Compass
Making America Sick — Part 4 of 4: The Fight Back
Share this:


Not Every Collapse Happens in Public
 Not Every Collapse Happens in Public
Not Every Collapse Happens in Public
Not every failure looks like a tent on a sidewalk.
Some of it happens quietly.
In apartments.
In classrooms.
In lives that, from the outside, still look like they’re moving forward.
There’s a tendency to separate things.
Homelessness over here.
Mental health over there.
Addiction somewhere else.
As if they’re different problems.
But they’re often just different points along the same path.
And not everyone reaches the visible end of it.
Some people fall apart long before that.
Without ever becoming part of the public conversation.
Even when there are signs, they’re easy to miss.
Or easy to misread.
Or easy to put off dealing with until later.
Because most people aren’t trained to recognize what they’re looking at.
And even if they are, they often don’t know what to do next.
So moments pass.
Windows close.
And what could have been interrupted… isn’t.
Afterward, there’s reflection.
Looking back. Connecting dots. Seeing things more clearly than they were at the time.
That happens more often than people talk about.
But even that awareness doesn’t automatically translate into something usable.
It doesn’t create a system.
It doesn’t create a path others can follow.
It just becomes another isolated experience.
That’s the pattern again.
Pieces that exist.
But don’t connect.
We tend to think of intervention as something formal.
Something that belongs to institutions, professionals, or systems.
But those systems are often hard to access, hard to navigate, or already overwhelmed.
So people are left in a kind of in-between space.
They can see something isn’t right.
But they don’t have a clear way to act on it.
And just like with the visible side of the problem, that space doesn’t stay empty.
It fills with delay.
With uncertainty.
With missed chances.
Not because people don’t care.
But because nothing around them is structured in a way that helps them act in time.
That’s a different kind of gap.
Less visible.
But just as real.
And just like the one we can see every day, it raises a similar question:
If the pieces are already there…
why don’t they come together in a way that actually works?

Share this:



Addressing Mental Health – “A Practical Approach:”
A Practical Approach: When Something Obvious Isn’t Being Done
There’s a lot of noise right now.
Wars. Elections. Markets. Politics layered on top of politics. Everyone talking, few people listening. Most of it feels unstable. Most of it feels out of reach.
And maybe that’s part of the problem.
Because while we’re all focused on the big, complicated, unsolvable things… there are problems sitting right in front of us that aren’t complicated at all.
They’re just not being picked up.
Addiction treatment is one of them.
Not addiction in isolation—because addiction is often the visible problem. The root often lies in untreated or poorly managed mental health challenges. But addiction is treatable. It’s measurable. Interventions can work. And it’s where we can actually make a difference.
We see it everywhere. In cities, small towns, emergency rooms, police calls, families trying to hold together. People falling through the cracks of systems that were supposed to catch them.
We’ve known this for years. Studied it. Funded it. Debated it. Reframed it. Turned it into policy arguments, budget fights, election talking points.
And still—it sits there.
Not solved. Not improving in any meaningful, consistent way.
Just… managed.
Part of the reason is that we’ve treated it like a political problem. Something to be argued over. Something funded or defunded depending on who’s in charge. Something that shifts direction every few years without building real continuity.
But addiction doesn’t wait for elections. It doesn’t follow politics. And this doesn’t feel like a political problem anymore.
It feels like a systems problem.
Systems problems—when they’re clear enough—can be built differently.
This isn’t about overhauling healthcare. It’s not about rewriting insurance laws or building another layer of bureaucracy.
It’s simpler than that.
It’s about creating places where people can go when they’re not okay—and actually get help for the things we can treat.
Structured help. Humane help. Recovery-focused help.
Places designed from the beginning to focus on outcomes, not billing cycles. Where addiction is addressed alongside the underlying mental health context. Where accountability is measured by whether people stabilize, recover, and return to life with some form of independence.
Right now, we spend an extraordinary amount of time and energy reacting to crises after they’ve already spilled out.
Emergency response. Law enforcement. Crisis management.
All necessary. None designed to fix the root.
The quieter question is whether we’re willing to build something that works before people reach that point.
This isn’t impossible.
It’s neglected.
And sometimes the difference between the two is simply whether someone decides to pick it up.
Share this:

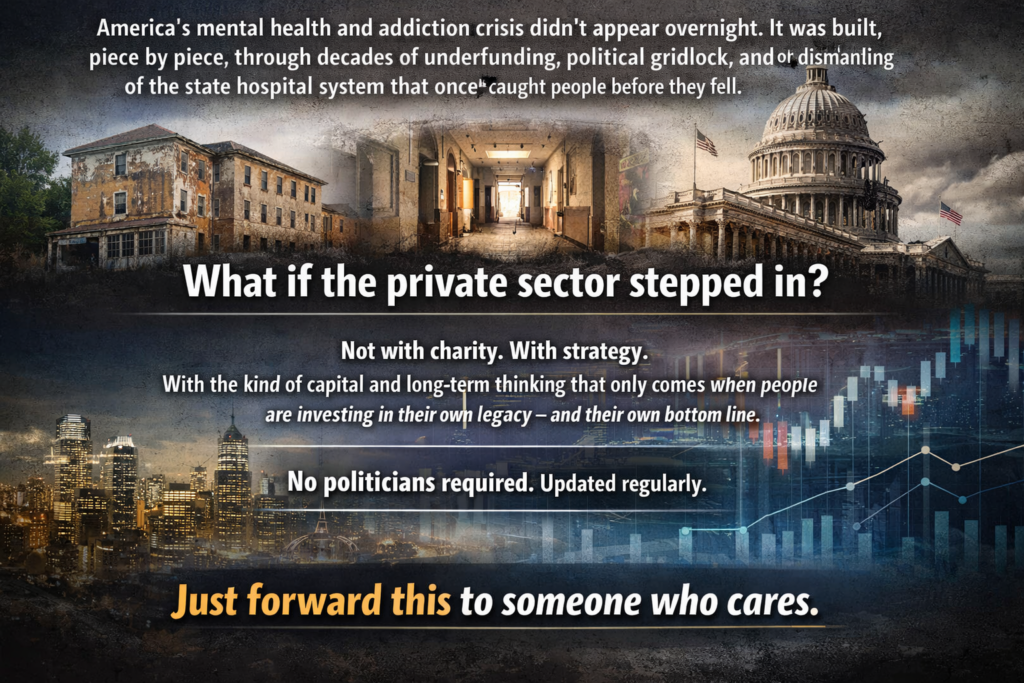
A Pivot Opportunity on America’s Mental Health Crisis – Redirecting Priorities from Endless War
Elon,You’ve already highlighted failures in mental health policy—deinstitutionalization left untreated severe cases on the streets, fueling homelessness, addiction, crime, and chaos (your “Make Asylums Great Again” posts in Feb 2026 nailed the critique of that 20th-century cost-cutting disaster). You’ve been open about personal struggles too (prescription ketamine for dark states, calling out “mental rabies” in violent offenders who need containment/treatment, not release).
The current hypocrisy is glaring and worsening: The Iran war (started late Feb 2026) is burning ~$1 billion/day (Pentagon briefed Congress on $11.3B+ in first 6 days; estimates now push $12–18B+ cumulative by mid-March, per CSIS/Reuters/NYT). That’s endless foreign escalation with no clear end, spiking gas prices and hurting Americans at home—while behavioral health funding gets squeezed (billions cut/reversed in SAMHSA grants under recent efficiencies).
A subtle distance from the current admin’s trajectory (less close proximity to avoid shrapnel from backlash) could open huge ground for you to lead on this domestically. Champion modern psychiatric treatment centers/recovery campuses (avoid “asylums” stigma—frame as humane, evidence-based facilities with safeguards, voluntary where possible, mandatory for severe threats). Tie it to protecting families/communities from exploitation, trauma, addiction cycles—subtly “shines” your image amid any lingering noise (e.g., old Epstein file smears).
Bring in Bezos, Zuckerberg, Ellison (Oracle) for a consortium: Announce an initial $19.5B fund (roughly 2–3 weeks of current war burn—people can do the math). Position it as:
-
Not replacing DEA street-level enforcement (that’s federal law job).
-
Funding treatment infrastructure: beds, crisis units, integrated SUD/mental health care, recovery housing, peer programs.
-
“Giving back”—this money originated from American taxpayers; redirecting a fraction to heal at home instead of endless abroad conflicts.
You have the platform (X), cash, and disruption cred to make this viral and bipartisan—addressing blue-city street crises and rural opioid/mental health gaps without heavy ideology. It aligns with your existing views, scales like your big missions, and could force national conversation/pressure for reallocations.
Worth considering? The timing (lame-duck dynamics, midterm/economic pain building) might be right.
No pressure—just an idea from a purple independent who’s tired of misplaced priorities.
@elonmusk – worth considering?

Making America Sick — Part 4 of 4: The Fight Back
If you have read this far and are feeling the particular kind of helplessness that comes from watching something important being dismantled by someone who cannot be reasoned with, this part is for you.
Because the resistance is real, it is organized, and some of it is winning.
The most important thing to understand is that Kennedy overplayed his hand legally, repeatedly, and the courts have noticed. He did not just pursue aggressive policy changes, he pursued them sloppily, skipping the procedural requirements that exist precisely to prevent any single person from unilaterally rewriting public health infrastructure. That sloppiness has created legal openings that are now being used effectively.
In March 2026 a federal judge in Massachusetts sided with the American Academy of Pediatrics and blocked Kennedy’s overhaul of the CDC’s vaccine advisory committee, the one he had stacked with skeptics after firing all 17 original members. The judge invalidated votes the reconstituted panel had already taken, including decisions to downgrade hepatitis B and COVID recommendations. More significantly, the same ruling found that the CDC had exceeded its legal authority when it unilaterally reduced the childhood vaccine schedule from 17 to 11 vaccines in January, because it did so without going through the proper advisory process. The mechanism Kennedy used to do the most damage to vaccine policy is the same mechanism that is now being used to undo it.
The states have mobilized in ways that matter. Fifteen states have sued to rescind the new vaccine schedule entirely and dismantle Kennedy’s replacement advisory committee. Nineteen states and the District of Columbia are separately fighting the HHS restructuring and mass layoffs on constitutional grounds, arguing the administration violated the separation of powers and the appropriations clause, essentially that Kennedy dismantled agencies Congress had funded and mandated without the legal authority to do so. A judge has already blocked further reorganization while that case proceeds. These are not symbolic lawsuits. They are methodical, well-resourced legal challenges built on solid procedural ground, and they are advancing.
Perhaps the most quietly encouraging development is what the medical establishment itself has done. When Kennedy changed the vaccine schedule, major hospital systems and clinicians across the country simply ignored it. The American Academy of Pediatrics published its own independent vaccine schedule, declaring the federal process no longer credible, and told its members to follow that instead. This matters more than it might seem. The federal government can change its recommendations, but it cannot force pediatricians to follow them. The professional infrastructure of American medicine, the societies, the hospitals, the training programs, the peer review systems, is largely intact and largely in open rebellion against what Kennedy is doing. That infrastructure is where the actual practice of medicine happens, and it is not waiting for federal permission to protect children.
Were the signs obvious? Yes. Could this have been prevented? Yes. Did it happen purely because of politics? Yes. But we also knew who Robert F. Kennedy Jr. was before he was confirmed, and we knew he was Trump’s chosen instrument for reshaping American public health. That makes all of us who watched and waited at least a little complicit in the complacency that allowed it to happen.
Casting blame now doesn’t cure a child with measles or restore a cancer research grant. It doesn’t rebuild the institutional knowledge that walked out the door with the scientists who were fired. The courts are working, and working effectively, but they are slow by design. The best and most immediate course of action is the one closest to home, your doctor, your pediatrician, your state legislature, your voice used early rather than late.
We knew. Now we act.
Know the insurance cliff and act before it hits. Major insurers pledged to keep covering the old vaccine schedule through end of 2026. That pledge expires in December. Before then, contact your state insurance commissioner and ask specifically what protections your state is putting in place to ensure continued vaccine coverage after the federal schedule changes. If your state has not addressed this, say so publicly and say it to your state legislators by name. This is the kind of specific, time-bound pressure that actually moves state government.
Talk to your pediatrician directly. Ask them which schedule they are following. The answer in most cases will be the American Academy of Pediatrics schedule, not the federal one. But parents who don’t ask won’t know, and parents who don’t know may make decisions based on federal guidance that their own doctor has already rejected. This is a conversation that takes five minutes and could matter enormously.
Support the organizations doing the legal work. The American Academy of Pediatrics, the American Public Health Association, and American Oversight are carrying the heaviest load in court right now. They are nonprofit organizations fighting well-funded federal legal teams. They need resources and they need visibility. Sharing their work, citing their findings, and donating if you are able is not performative, it is direct support for the people holding the legal line.
Pay attention to your state legislature. Anti-vaccine activists are already moving into statehouses to use the federal schedule changes as leverage to loosen school vaccine requirements. This is happening right now in Florida and Texas and it will spread. School board meetings and state legislative hearings are where this battle will be won or lost at the community level, and they are chronically under-attended by the people who would push back. You do not have to become an activist. You have to show up once and bring two people who agree with you.
Understand what is reversible and what isn’t. The legal framework to restore the vaccine schedule exists and is being actively pursued. The court victories so far suggest it is achievable. What is harder to reverse is the institutional knowledge that walked out the door with the fired scientists, the research that wasn’t funded, the surveillance systems that went dark, and the public trust that eroded while the outbreaks spread. Those are long term repair projects that will require sustained political will across multiple administrations. That is not a reason for despair. It is a reason to vote in every election at every level with health policy as a primary consideration, and to say so out loud when you do.
The measles outbreak will not be the last consequence we see from what has happened at HHS over the past year. The cancer research that wasn’t funded will show up in treatment outcomes years from now. The children who didn’t get vaccinated because their parents received confusing guidance from the federal government will be vulnerable in ways that won’t be visible until the next outbreak arrives. The damage has a long tail.
But so does the resistance. The courts are not done. The states are not done. The medical establishment is not done. And the accumulated weight of evidence-based medicine, built over more than a century by people who understood that complexity requires sustained attention rather than simple answers, does not disappear because one man with a broken compass was handed the keys for a few years.
He was given those keys through a political transaction. They can be taken back through a democratic one.
That is not optimism. That is how the system is supposed to work, and right now, imperfectly and under enormous pressure, it is working.
Pay attention. Show up. Talk to your pediatrician.
The burger and the shake are not going to fix this either.
Share this:
Like this: