



















































































































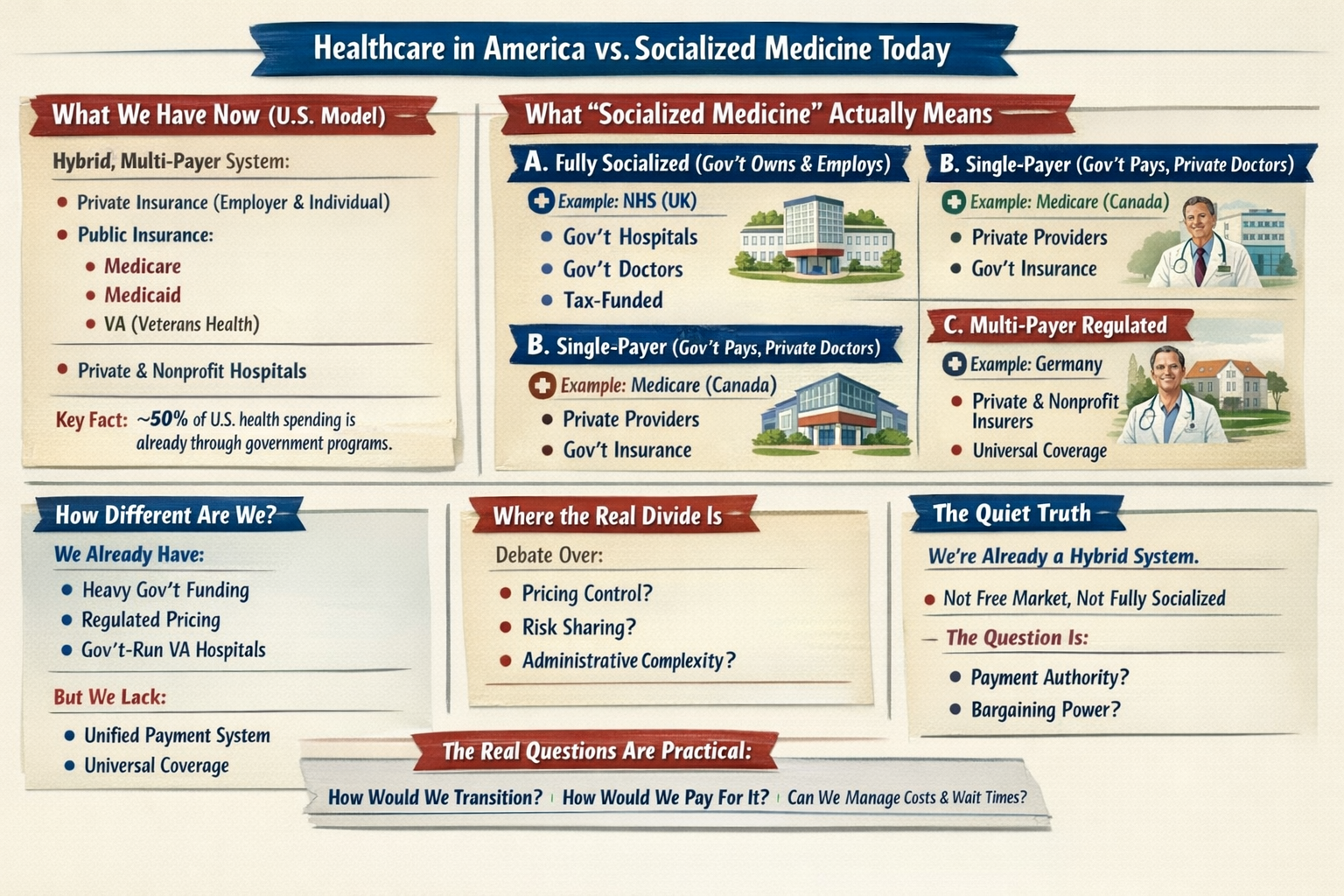
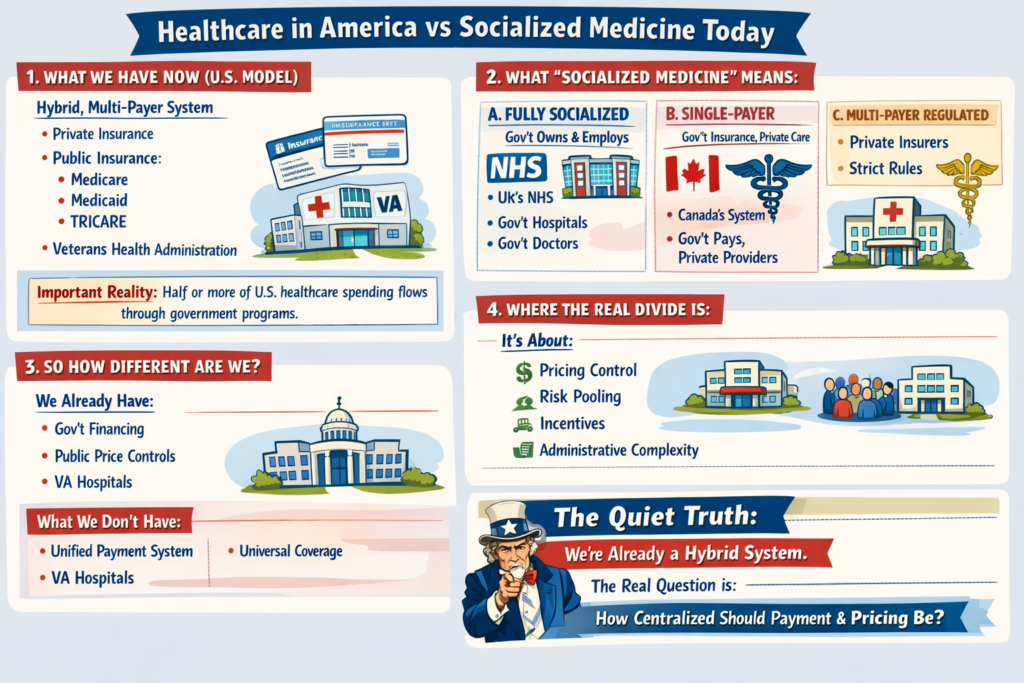
Healthcare in America vs Socialized Medicine Today
1. What We Have Now (U.S. Model)
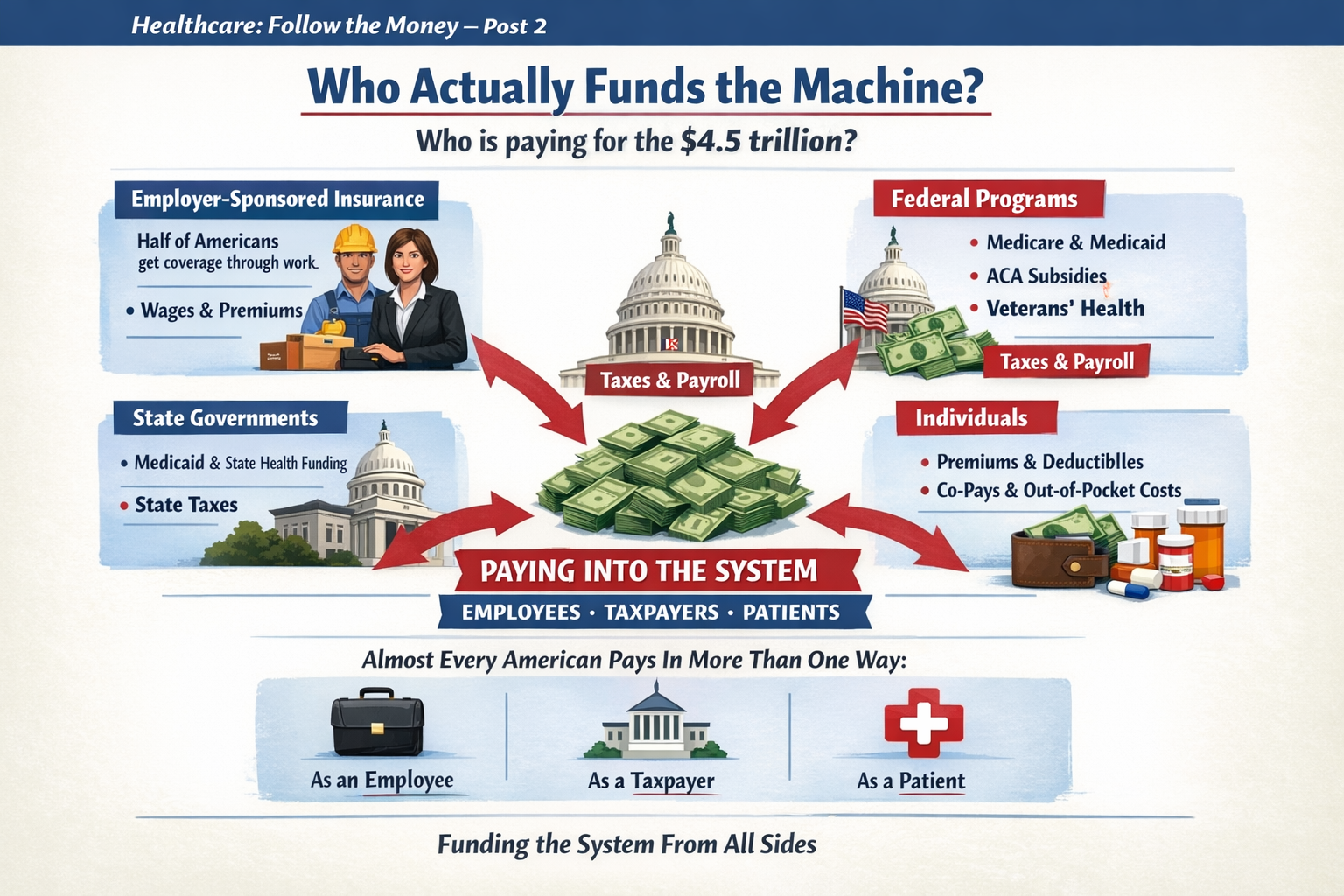
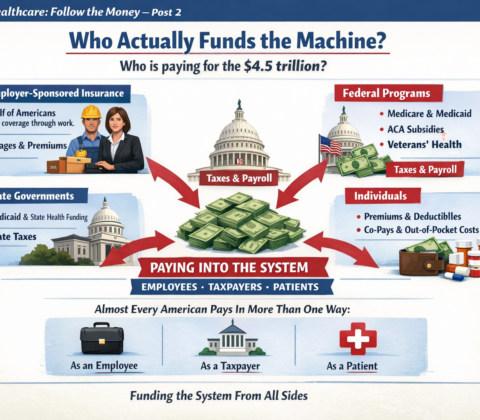
The U.S. system is a hybrid, multi-payer system:
-
Private insurance (employer-based and individual market)
-
Public insurance:
-
Medicare
-
Medicaid
-
TRICARE
-
Veterans Health Administration
-
-
Private hospitals (mostly nonprofit, some for-profit)
-
Private physician practices (increasingly consolidated)
Important reality:
Roughly half or more of U.S. healthcare spending already flows through government programs. We are not a pure market system. We are a complex blend.
2. What “Socialized Medicine” Actually Means
People often use “socialized” loosely. There are actually three different models internationally:
A. Fully Socialized (Government Owns & Employs)
Example: National Health Service in the UK
-
Government owns hospitals
-
Doctors are government employees
-
Government sets budgets directly
-
Care funded through taxes
That’s true “socialized medicine.”
B. Single-Payer (Government Pays, Private Providers Deliver)
Example: Medicare (Canada’s system)
-
Private hospitals & doctors
-
Government is the main insurer
-
One public payment system
-
Funded via taxes
This is not government-run hospitals — it’s government-run insurance.
C. Multi-Payer Regulated System
Example: Statutory Health Insurance
-
Private and nonprofit insurers
-
Strict national rules
-
Price controls
-
Universal coverage mandate
3. So How Different Are We?
Structurally:
-
We already have heavy government financing.
-
We already regulate pricing in public programs.
-
We already operate large government-run care systems (VA hospitals).
-
We already subsidize private insurance through tax exclusions.
What we don’t have:
-
A unified payment structure
-
National price controls across the board
-
Universal automatic coverage
-
Simplified billing
The biggest structural difference isn’t just “who pays.”
It’s:
-
Fragmentation
-
Administrative layering
-
Pricing freedom in private markets
-
Employment-tied insurance
4. Where the Real Divide Is
The debate isn’t simply:
Private vs Socialized.
It’s about:
-
Who controls pricing?
-
How risk is pooled?
-
How incentives are aligned?
-
How much administrative complexity is tolerated?
Even a “socialized” system still rations care — just differently (wait times vs cost-sharing).
Even our current system has price controls — just unevenly applied.
5. If the U.S. “Moved Toward Socialized” — What Would Actually Change?
Not necessarily hospital ownership.
More likely changes would include:
-
Centralized bargaining power
-
Uniform reimbursement rates
-
Elimination of employer-based insurance
-
Tax-based funding instead of premium-based funding
-
Dramatically reduced administrative overhead
-
Reduced insurer role
The money flow changes.
The power centers shift.
Administrative structure simplifies.
But doctors would still practice medicine.
Hospitals would still exist.
Care would still be rationed — just through different mechanisms.
6. The Quiet Truth
We are already halfway between models.
The U.S. system is not a free market.
It is not socialized.
It is a layered hybrid with competing incentives.
The question isn’t:
“Would we become socialized?”
The real question is:
“How centralized do we want payment and pricing authority to be?”
That’s a structural debate — not just a funding debate.
To go deeper, we have to explore:
-
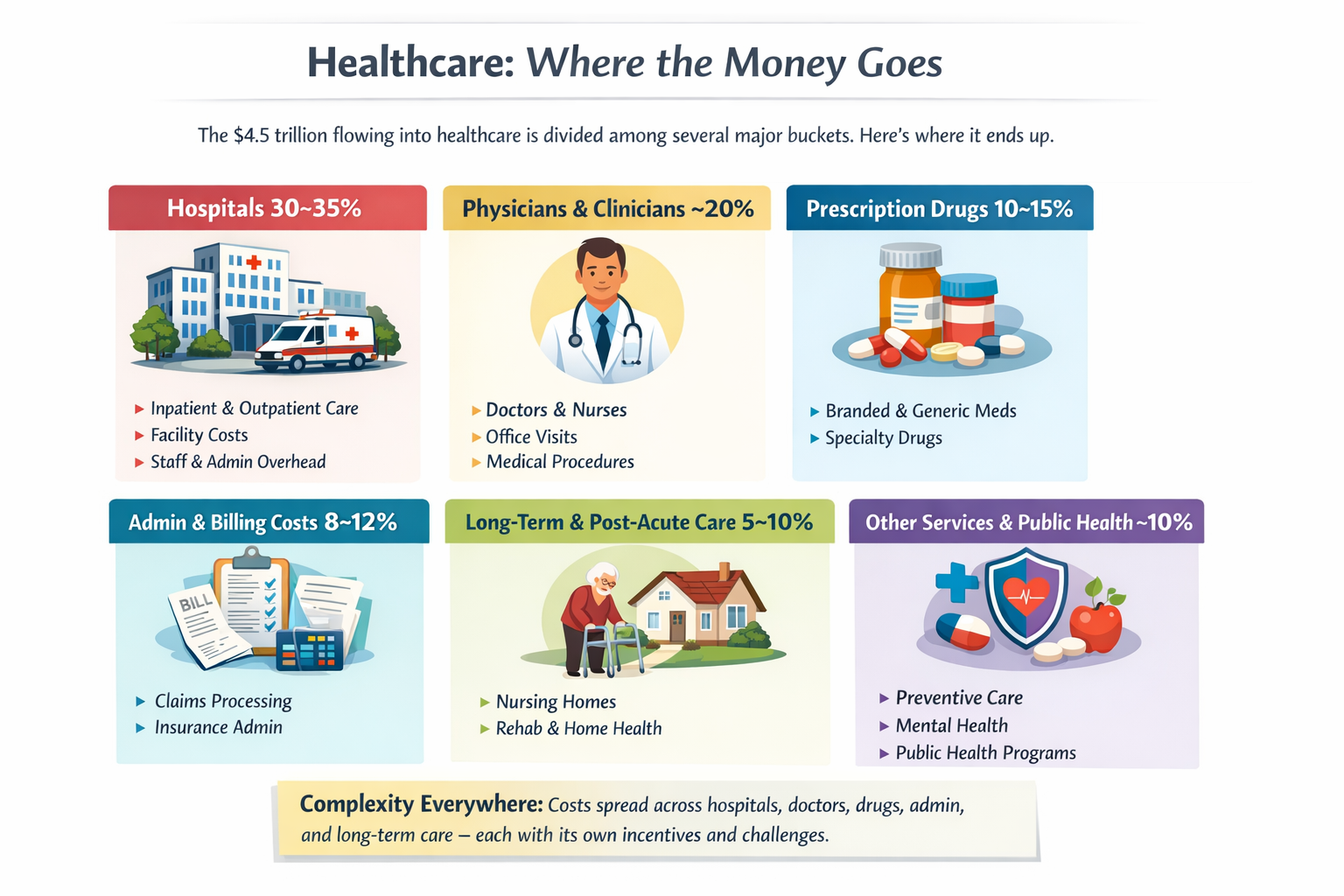
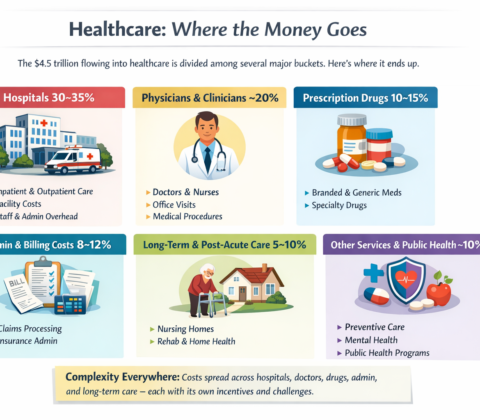
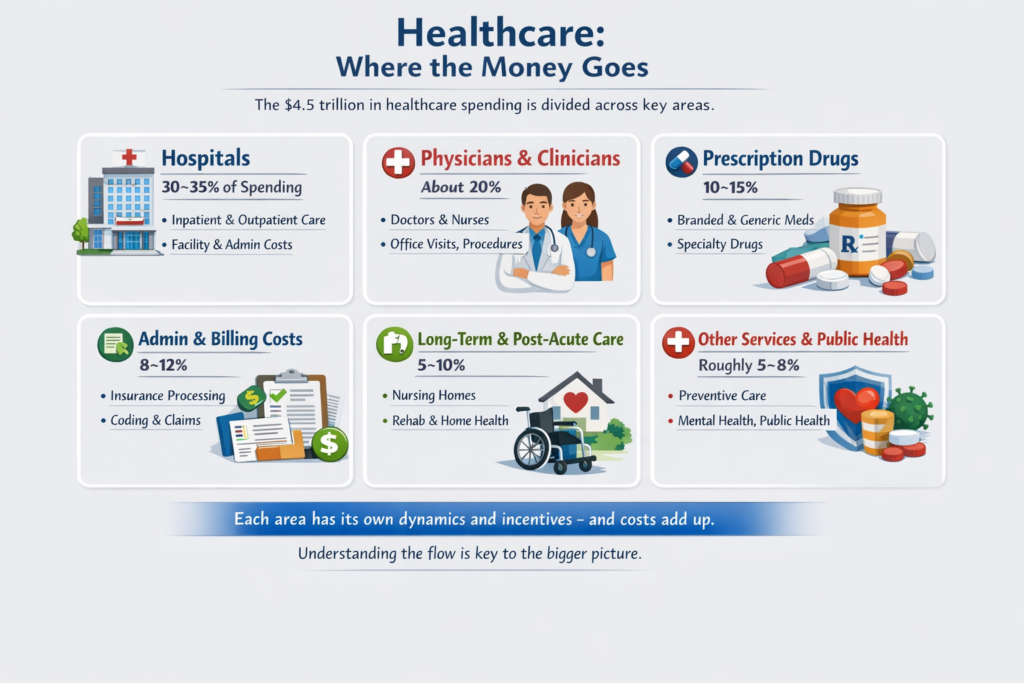
What would actually happen to costs?
-
What happens to innovation?
-
What happens to wait times?
-
Or what a realistic transition would look like?
The real questions aren’t ideological. They’re mechanical:



































































































































Impeach Him, Impeach Him, Well Maybe we Hold Off On That – Piece 2: Why Not Impeaching Might Be the Smarter Move – Video
Come the midterms, I’m pretty sure the Democrats gain control, good chance both houses, and then it’s impeachment time, right? Right? Right?
Well, here’s the thing. Yes, it could be impeachment time. But should it be? Big question. Very big question.
Until the midterms, unless Trump really alienates his own MAGA Congress, all the Democrats can do is make a bunch of noise. And, well, make a bunch of noise. I subscribe to a lot of Substack writers, left-leaning and right-leaning both, and every single one is “look what he did today, that’s an impeachable offense”, and then nothing happens the next day. Day after day. For the past year. It’ll make you crazy.
Worse are the attorneys, spouting law, and still, day after day, nothing happens. Trump himself said his power is absolute until proven otherwise. Well. Will somebody actually prove it?
======================================
You wouldn’t be running a candidate against the sitting president in 2028, you’d be running against a legacy. Vance may be on the ticket, but he won’t be the incumbent, and he’ll face real opposition from inside his own party, whatever that party even is by then. MAGA, MAGA 2.0, or Vance quietly rebranding himself as someone who was a Republican all along, working from the inside, Benedict Vance, unless Rubio beats him to it.
So: to impeach, or not to impeach. Maybe that’s the question we put to Congress before they decide it on their own. After all, they work for us.
This is just a prelude to an upcoming 4 part series on what’s to gain by impeachment and what’s to gain by NOT impeaching Trump. It’s not an easy decision, especially if we want actual Government, Not REVENGE tactics.
Share this:
Like this: