



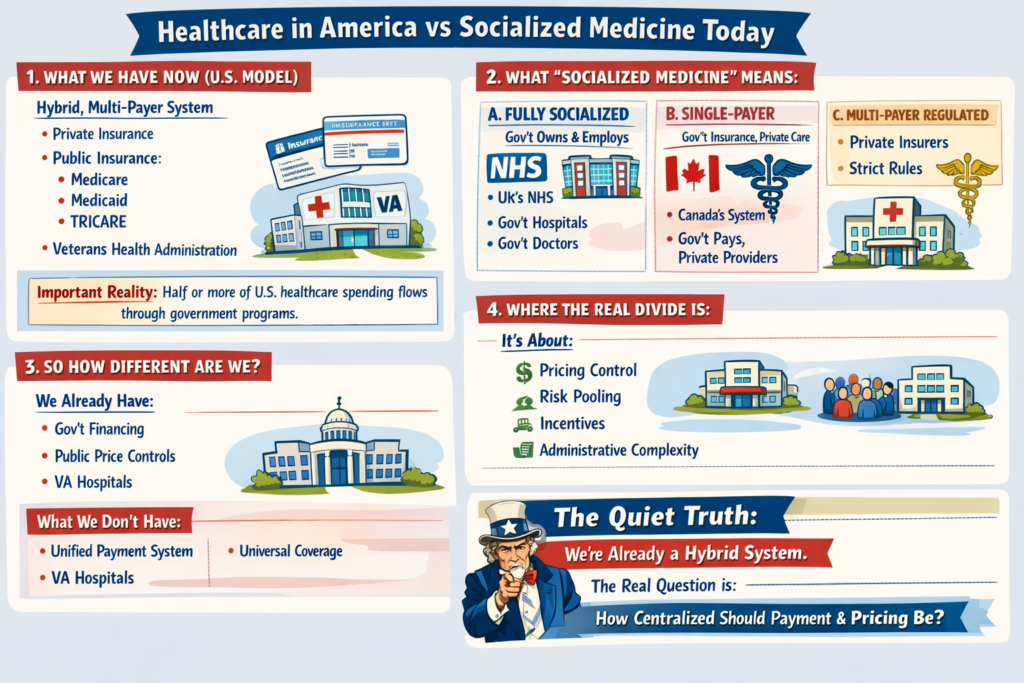
Healthcare in America vs Socialized Medicine Today
1. What We Have Now (U.S. Model)
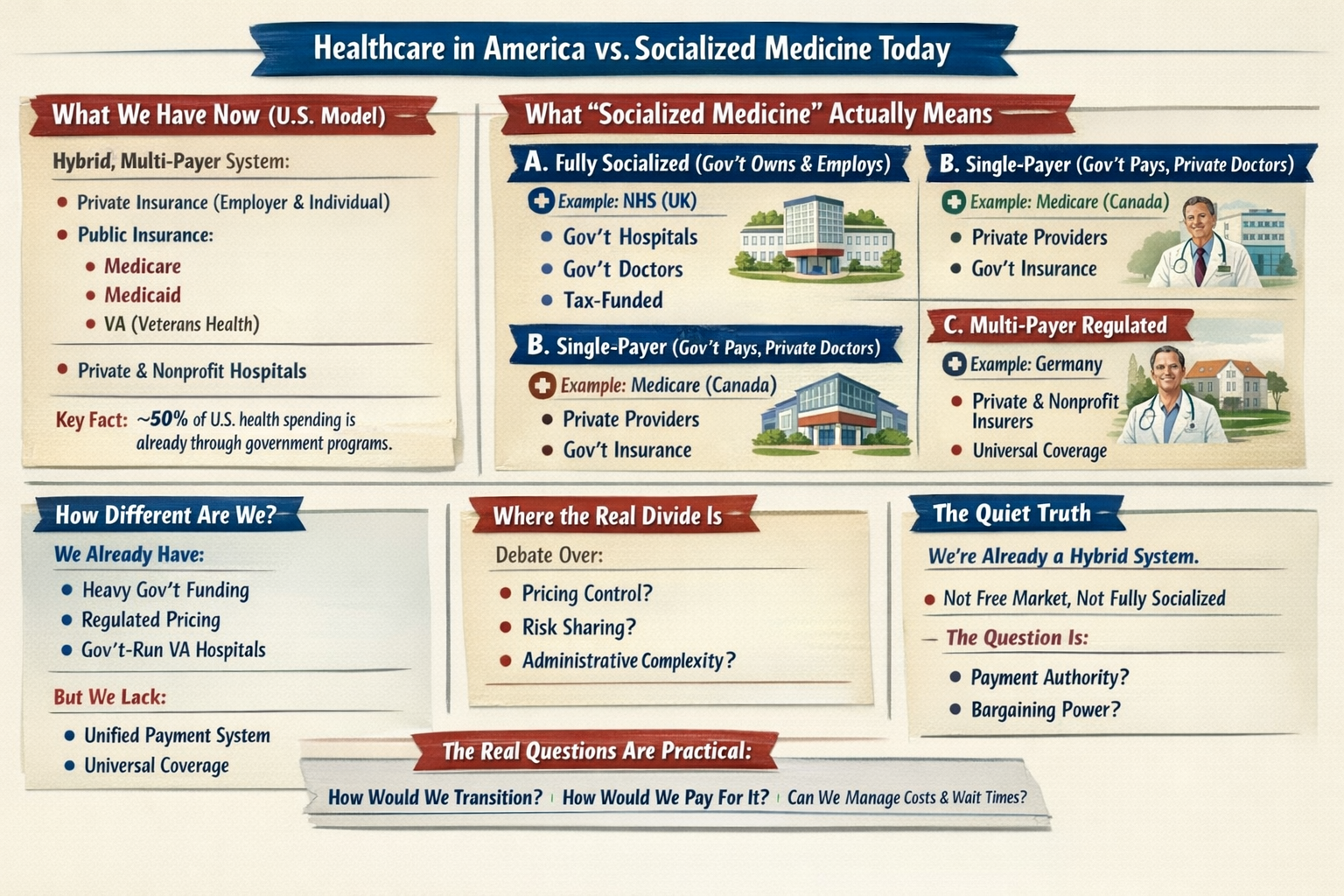
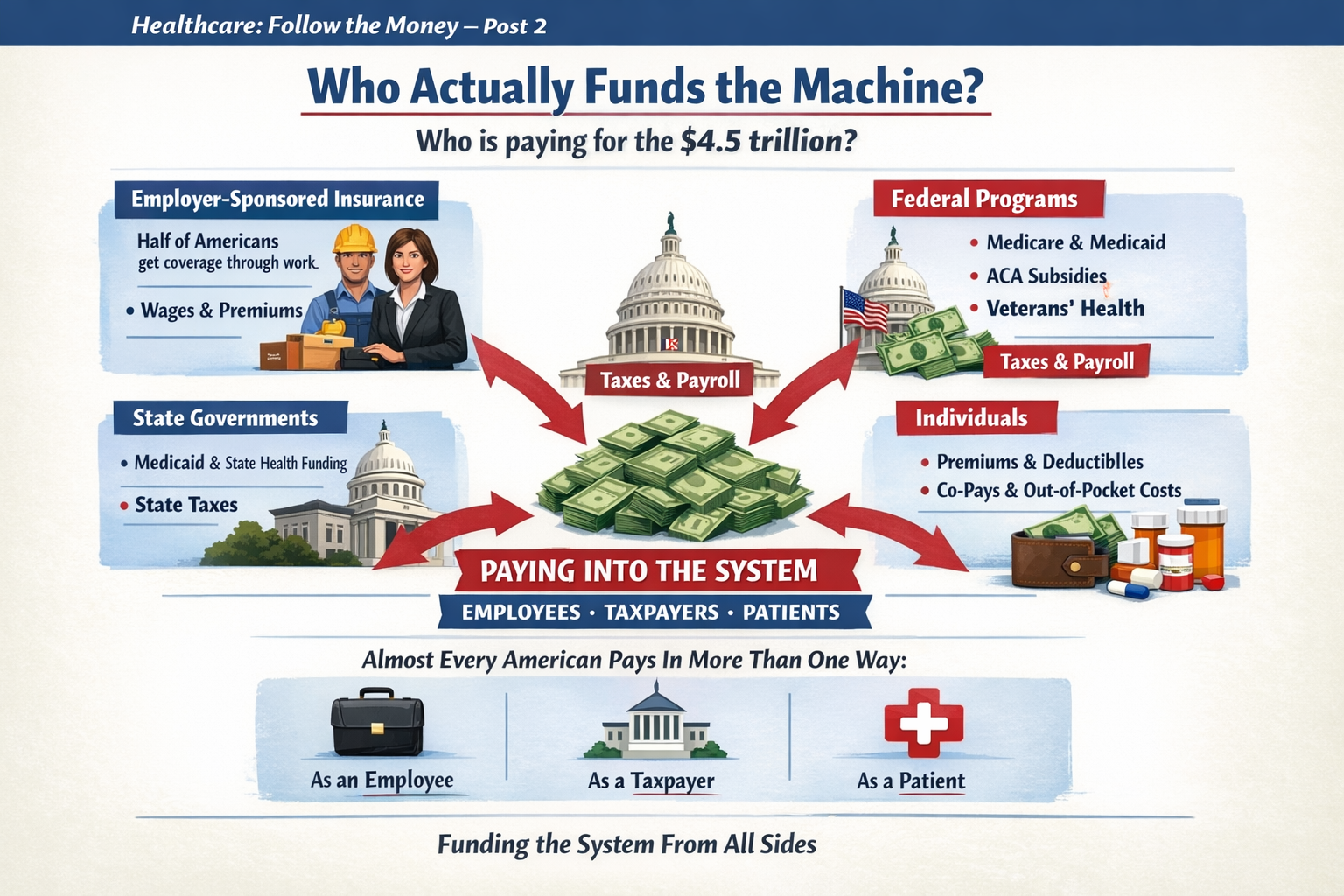
The U.S. system is a hybrid, multi-payer system:
-
Private insurance (employer-based and individual market)
-
Public insurance:
-
Medicare
-
Medicaid
-
TRICARE
-
Veterans Health Administration
-
-
Private hospitals (mostly nonprofit, some for-profit)
-
Private physician practices (increasingly consolidated)
Important reality:
Roughly half or more of U.S. healthcare spending already flows through government programs. We are not a pure market system. We are a complex blend.
2. What “Socialized Medicine” Actually Means
People often use “socialized” loosely. There are actually three different models internationally:
A. Fully Socialized (Government Owns & Employs)
Example: National Health Service in the UK
-
Government owns hospitals
-
Doctors are government employees
-
Government sets budgets directly
-
Care funded through taxes
That’s true “socialized medicine.”
B. Single-Payer (Government Pays, Private Providers Deliver)
Example: Medicare (Canada’s system)
-
Private hospitals & doctors
-
Government is the main insurer
-
One public payment system
-
Funded via taxes
This is not government-run hospitals — it’s government-run insurance.
C. Multi-Payer Regulated System
Example: Statutory Health Insurance
-
Private and nonprofit insurers
-
Strict national rules
-
Price controls
-
Universal coverage mandate
3. So How Different Are We?
Structurally:
-
We already have heavy government financing.
-
We already regulate pricing in public programs.
-
We already operate large government-run care systems (VA hospitals).
-
We already subsidize private insurance through tax exclusions.
What we don’t have:
-
A unified payment structure
-
National price controls across the board
-
Universal automatic coverage
-
Simplified billing
The biggest structural difference isn’t just “who pays.”
It’s:
-
Fragmentation
-
Administrative layering
-
Pricing freedom in private markets
-
Employment-tied insurance
4. Where the Real Divide Is
The debate isn’t simply:
Private vs Socialized.
It’s about:
-
Who controls pricing?
-
How risk is pooled?
-
How incentives are aligned?
-
How much administrative complexity is tolerated?
Even a “socialized” system still rations care — just differently (wait times vs cost-sharing).
Even our current system has price controls — just unevenly applied.
5. If the U.S. “Moved Toward Socialized” — What Would Actually Change?
Not necessarily hospital ownership.
More likely changes would include:
-
Centralized bargaining power
-
Uniform reimbursement rates
-
Elimination of employer-based insurance
-
Tax-based funding instead of premium-based funding
-
Dramatically reduced administrative overhead
-
Reduced insurer role
The money flow changes.
The power centers shift.
Administrative structure simplifies.
But doctors would still practice medicine.
Hospitals would still exist.
Care would still be rationed — just through different mechanisms.
6. The Quiet Truth
We are already halfway between models.
The U.S. system is not a free market.
It is not socialized.
It is a layered hybrid with competing incentives.
The question isn’t:
“Would we become socialized?”
The real question is:
“How centralized do we want payment and pricing authority to be?”
That’s a structural debate — not just a funding debate.
To go deeper, we have to explore:
-
What would actually happen to costs?
-
What happens to innovation?
-
What happens to wait times?
-
Or what a realistic transition would look like?
The real questions aren’t ideological. They’re mechanical:










































































































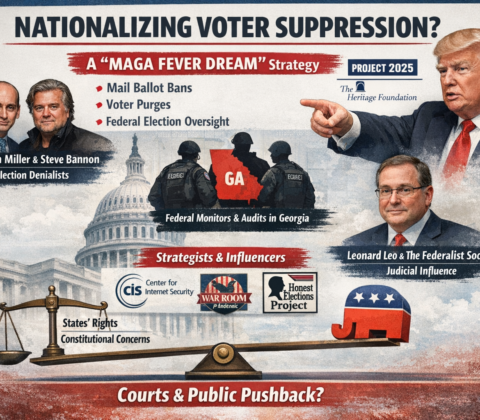
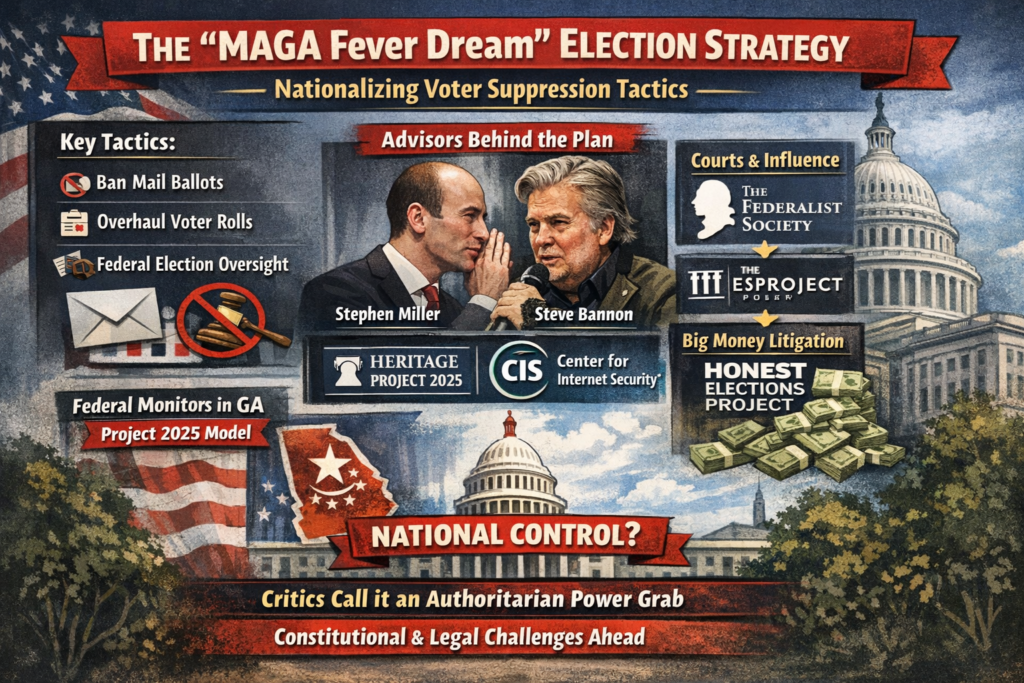
























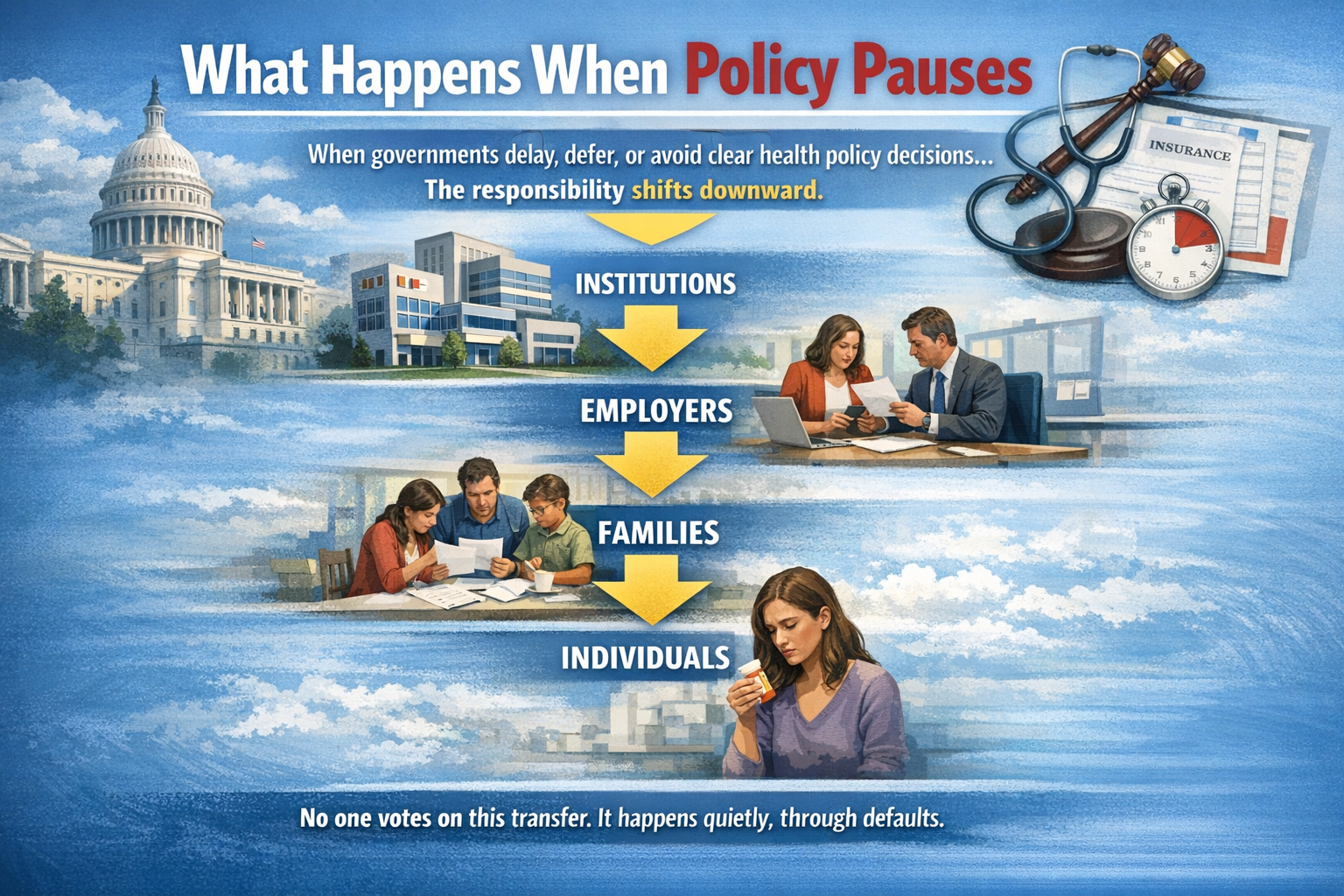



































































Protecting Your Voting Rights
Protecting voting rights is a fundamental aspect of American democracy, and your concern about potential executive overreach is valid given recent reports. While presidents have issued executive orders related to elections in the past, they don’t have unilateral authority to control how states run them, elections are primarily a state responsibility under the Constitution (Article I, Section 4), with Congress able to set or alter regulations for federal races. Any attempt to impose sweeping changes via executive order, especially if premised on unsubstantiated claims like foreign interference from past elections, would likely face immediate legal challenges and injunctions from federal courts, as happened with a similar order in March 2025.
Courts have repeatedly affirmed that such actions can’t override constitutional limits or state authority without clear statutory backing.
That said, litigation can take time, so proactive steps are key to safeguarding access to the ballot. Here’s what individuals and communities can do, based on established strategies from voting rights organizations:1. Stay Informed and Monitor Changes
Follow reliable sources for updates on election laws and any proposed executive actions. Organizations like the ACLU, Brennan Center for Justice, and League of Women Voters track voter suppression efforts and provide alerts.
Sign up for their newsletters or use tools like the Election Assistance Commission’s (EAC) website to check your state’s rules.
Track bills in Congress, such as efforts to restore the full protections of the Voting Rights Act of 1965 (e.g., the John R. Lewis Voting Rights Advancement Act), which could counter discriminatory changes.
The Act’s preclearance provision historically required federal approval for changes in states with discrimination histories, though it was weakened by the Supreme Court in 2013.
2. Register, Vote, and Help Others Do the Same
Ensure you’re registered and update your information if needed—use the National Voter Registration Act (NVRA) provisions, which allow registration at DMVs or online in many states.
Encourage friends, family, and neighbors to register early to avoid last-minute barriers.
Vote in every election, including primaries and locals, where turnout can influence who shapes voting rules. If mail voting or early voting is available in your state, use it to reduce reliance on Election Day logistics that could be disrupted.
Know your rights: Federal laws like the Voting Rights Act prohibit discrimination based on race, color, or language, and the Help America Vote Act (HAVA) ensures provisional ballots if your eligibility is questioned. If you face issues at the polls (e.g., intimidation or denial), report them immediately to the DOJ’s Voting Section or the Election Protection Hotline (866-OUR-VOTE).
3. Support Advocacy and Legal Efforts
Donate to or volunteer with groups fighting voter suppression, such as the NAACP Legal Defense Fund, Common Cause, or the Brennan Center. They file lawsuits to block unlawful changes and have successfully challenged past executive orders.
For instance, multiple courts blocked key parts of the 2025 election integrity order.
Push for state-level Voting Rights Acts, which some states have adopted to fill gaps left by federal weakenings.
Contact your state legislators to advocate for expansions like automatic voter registration or protections against purges.
4. Engage Civically and Build Community
Contact your members of Congress to oppose bills like the SAVE America Act if they create unnecessary barriers (e.g., strict proof-of-citizenship requirements), and support reforms like the Freedom to Vote Act for national standards on early voting and mail ballots.
Volunteer as a poll worker, watcher, or nonpartisan monitor through groups like the EAC or local election boards. This helps ensure transparency and can deter irregularities.
Join or form community groups to educate others—host voter registration drives or workshops on recognizing misinformation about elections.
5. Prepare for Potential Challenges
If an executive order is issued attempting to mandate things like nationwide voter ID, bans on mail voting, or federal oversight of state systems, expect rapid court action.
Advocacy groups are already poised to challenge them, arguing they exceed presidential authority and violate states’ rights.
In the meantime, focus on state-level protections, as federal overreach often gets enjoined quickly.
Document and report any suspicious activity, like voter purges or intimidation, to the FBI or state attorneys general.
Ultimately, the strongest defense is high participation and collective action—history shows that when voters mobilize, attempts to restrict access often fail. If things escalate, resources like the DOJ’s Civil Rights Division can provide enforcement.
Stay engaged, and remember that protections like the 14th, 15th, and 19th Amendments provide a solid foundation against discrimination.
Share this:
Like this: