


















































































We’ve traced the system from dollars to delivery, explored chronic disease, and examined rural pressures. Now we ask a crucial question: who actually benefits from the way the system is structured?
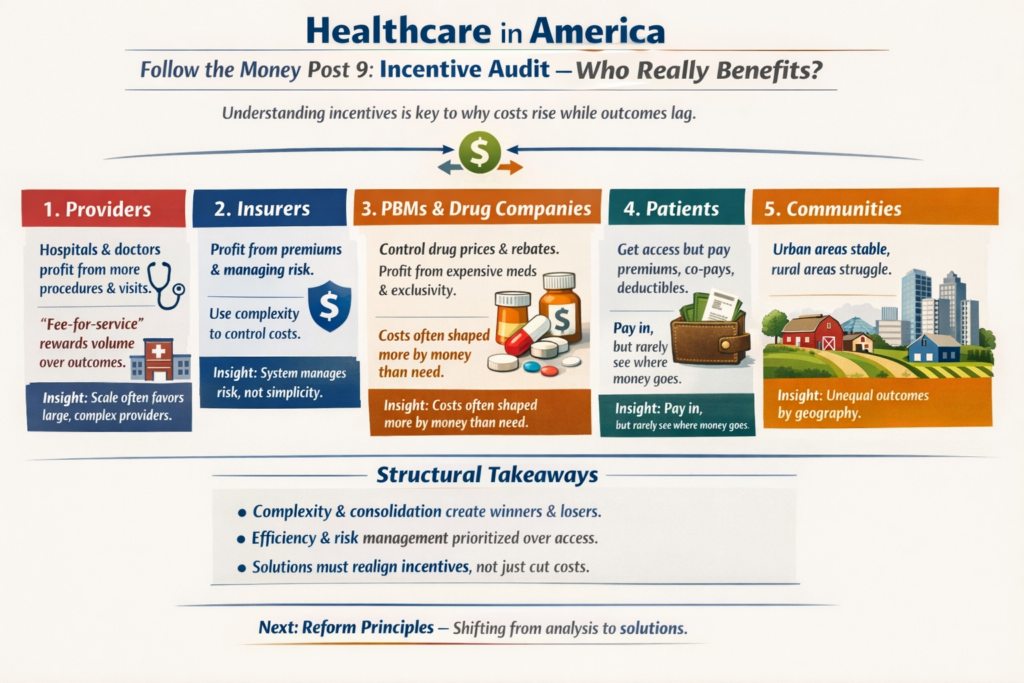
Understanding incentives is key to seeing why healthcare costs continue to rise, even when outcomes lag.
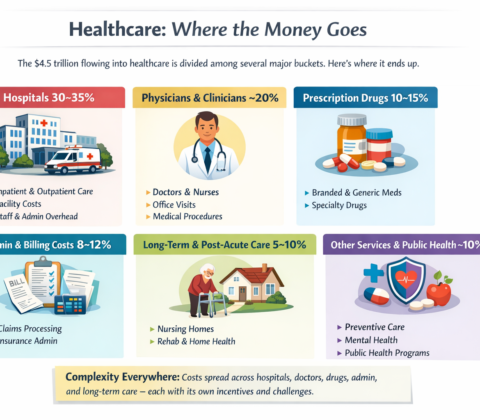
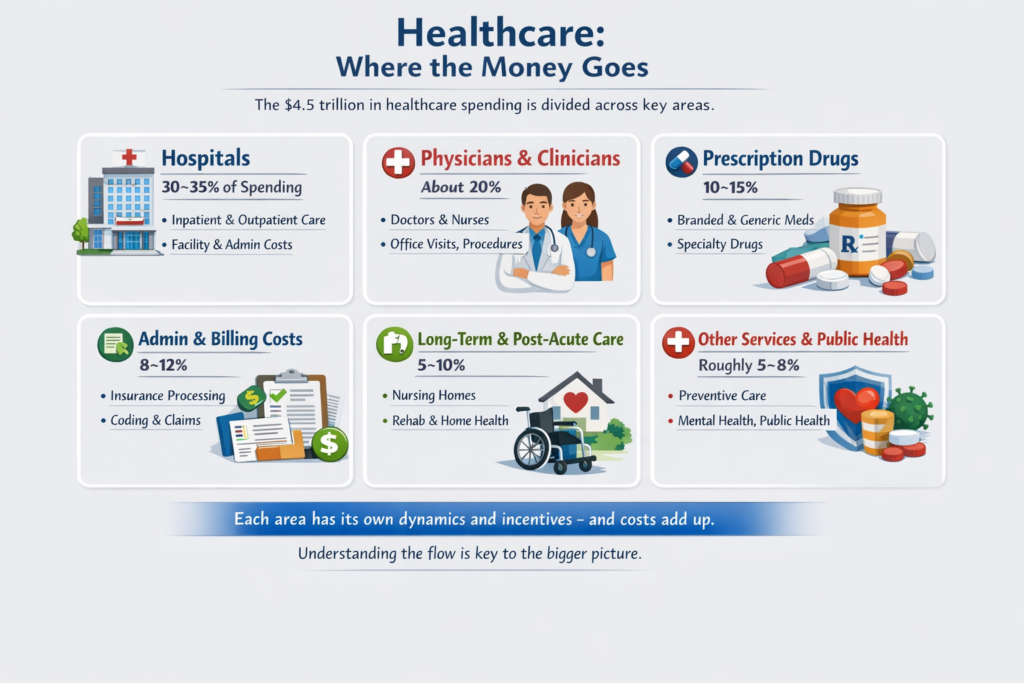
1. Providers
-
Hospitals and physician groups benefit when patients utilize services — more procedures, more visits, more tests.
-
Fee-for-service payment models reward volume rather than long-term outcomes.
-
Administrative complexity can create higher revenue for larger organizations that can manage it efficiently, leaving smaller providers struggling.
Insight: scale and complexity often favor larger, well-resourced providers.
2. Insurers
-
Insurance companies benefit from predictable revenue through premiums and from managing risk pools.
-
Complexity (deductibles, prior authorizations, network rules) allows insurers to control costs and reduce risk exposure.
-
Administrative layers are part of this management — they protect financial stability but also add friction for patients.
Insight: the system is designed to manage risk, not maximize simplicity.
3. Pharmacy Benefit Managers & Drug Manufacturers
-
PBMs negotiate prices and rebates, influencing which medications are accessible or costly.
-
Drug manufacturers benefit from high-cost specialty medications and brand exclusivity periods.
Insight: financial structures shape access and cost, sometimes more than clinical need does.
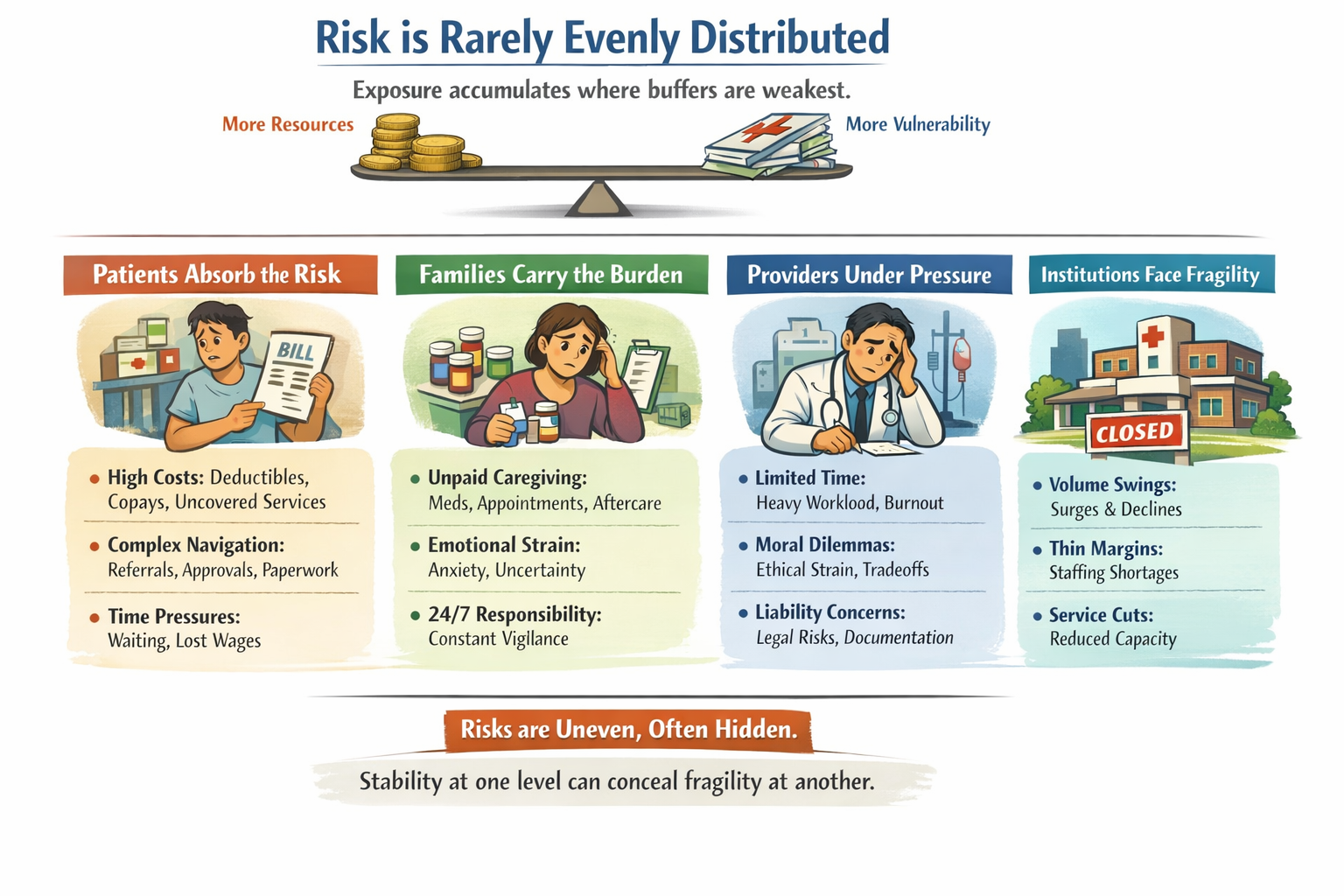
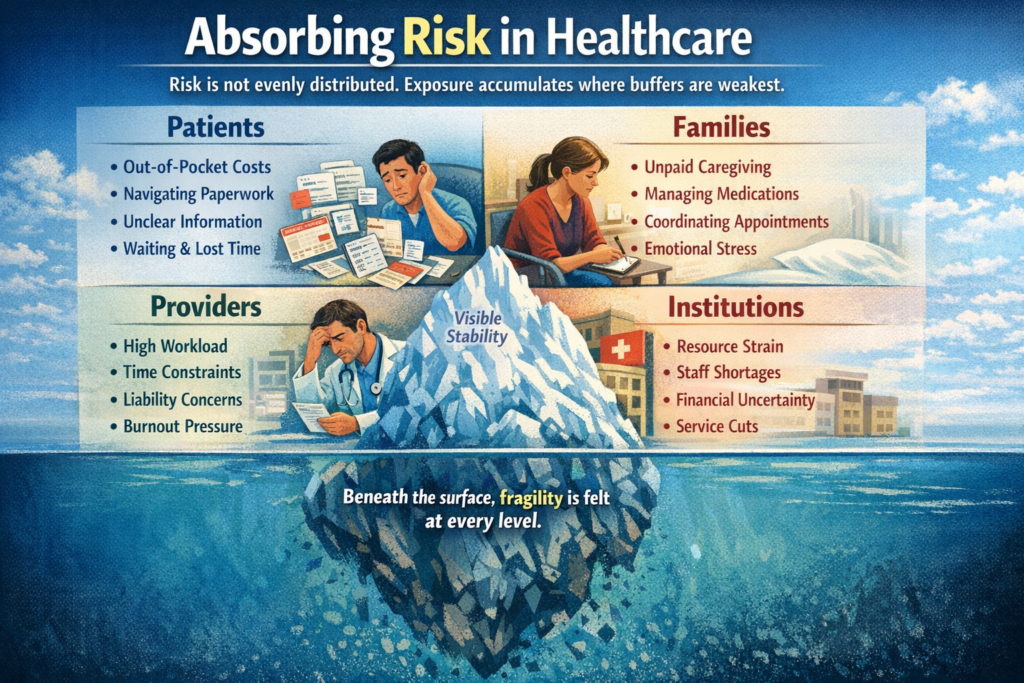
4. Patients
-
Patients benefit from insurance coverage, access to advanced care, and risk protection.
-
Yet they also bear the cost of complexity: premiums, deductibles, co-pays, travel for care, and confusing bills.
Insight: patients participate financially at multiple points but rarely see the full flow of funds, which reduces visibility and understanding.
5. Communities
-
Urban centers with high volumes and consolidated hospitals often maintain stable services.
-
Rural communities with low volumes and fewer resources are vulnerable to closures and service reductions.
Insight: structural scale advantages create unequal outcomes across geographies.
Structural Takeaways
-
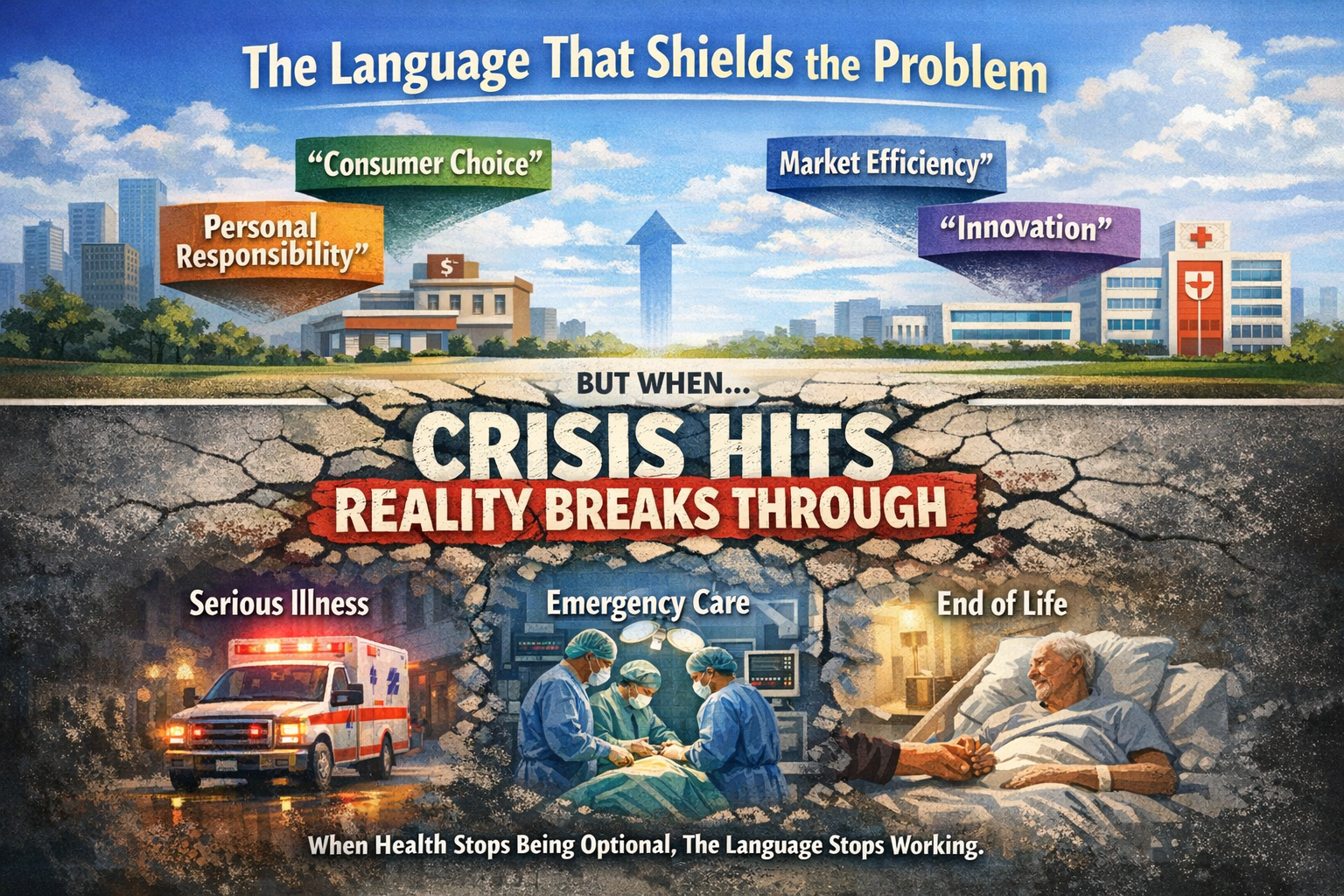
Complexity, consolidation, and financial engineering create winners and losers.
-
The system works for efficiency and risk management, but not always for access, affordability, or simplicity.
-
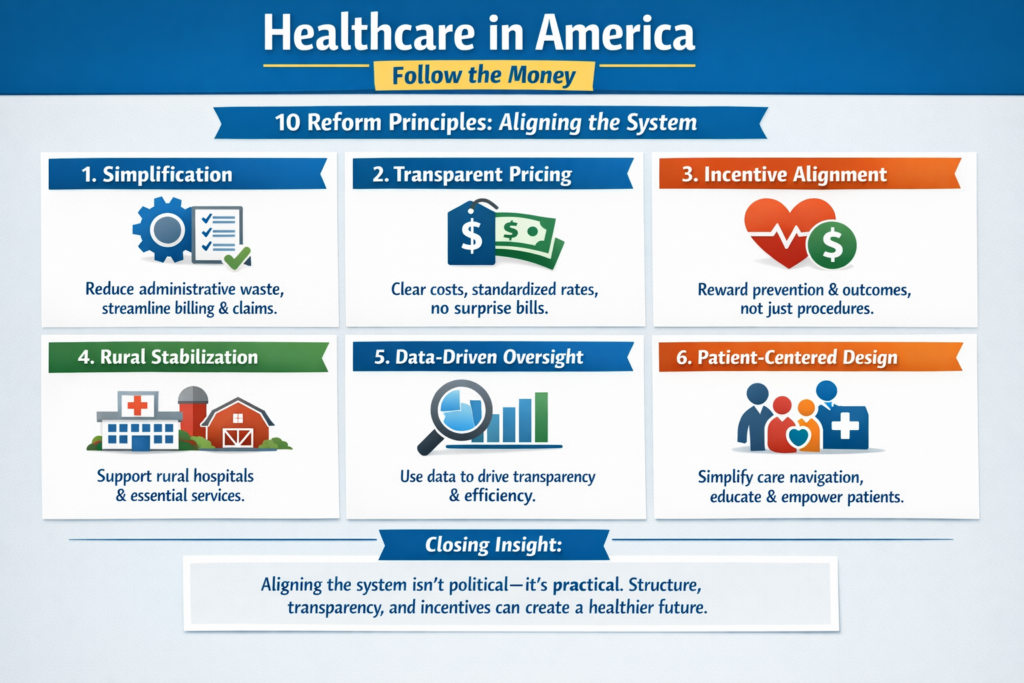
Understanding incentives is essential before discussing reform: any solution must realign motivations, not just cut costs.
Transition
With incentives mapped, we can now move to the final post — Reform Principles. Here, we shift from analysis to constructive thinking, outlining structural ideas that could reduce friction, improve access, and align incentives with health outcomes.