Healthcare in America, Follow the Money, Post 3, Where the Money Goes
Knowing who pays is only the start. To understand the system, we need to see where those dollars actually land.
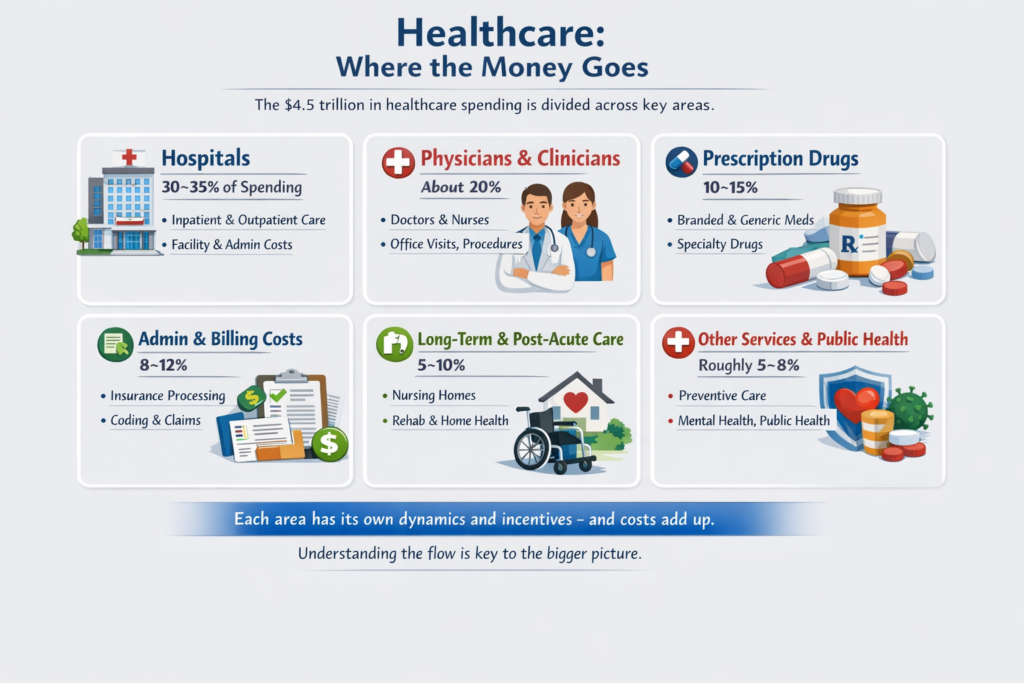
The $4.5 trillion flowing into healthcare doesn’t go to one place. It is split across several major buckets, each with its own dynamics and incentives.
1. Hospitals — Roughly 30–35% of Spending
Hospitals are the single largest cost center.
Inpatient care: surgeries, ICU, long stays
Outpatient care: ER visits, imaging, labs, procedures
Every additional layer adds cost, even if it doesn’t touch patient care directly.
2. Physicians & Clinicians — About 20%
Doctors, nurses, and other clinicians account for roughly one-fifth of total spending.
Compensation varies widely by specialty
Fee-for-service models often reward procedures over preventive care
Here, incentives shape behavior: more complex, billable procedures generate revenue, while counseling or preventive care may not.
3. Prescription Drugs — 10–15%
Prescription spending includes:
Branded drugs
Generics
Specialty medications
Price negotiation occurs through insurers and pharmacy benefit managers, but patients often experience unpredictability in costs, especially for high-cost or specialty medications.
4. Administrative & Billing Costs — 8–12%
One of the largest invisible drivers of cost:
Claims processing
Coding
Prior authorizations
Billing disputes
Studies show U.S. administrative costs are twice those of comparable countries, yet they do not directly improve patient care.
5. Long-Term & Post-Acute Care — 5–10%
Includes:
Nursing homes
Rehab facilities
Home health care
Population aging and chronic disease prevalence drive spending in this area.
6. Other Services & Public Health
The remainder covers:
Preventive care
Public health initiatives
Mental health services
Emergency preparedness
Small individually, but collectively essential.
Structural Insight
Looking at the buckets, one pattern emerges: complexity drives cost.
Hospitals and physician care dominate, but are themselves entangled with administrative and billing layers.
Drugs and specialized services add unpredictability.
Individuals and payers have little visibility into total flow.
The next step is tracing the flow of a single dollar — from paycheck to provider — to make the system tangible. That’s where things get almost counterintuitive, and where the first real tension appears between intention and outcome.


Comments are Disabled