Healthcare in America vs Socialized Medicine Today
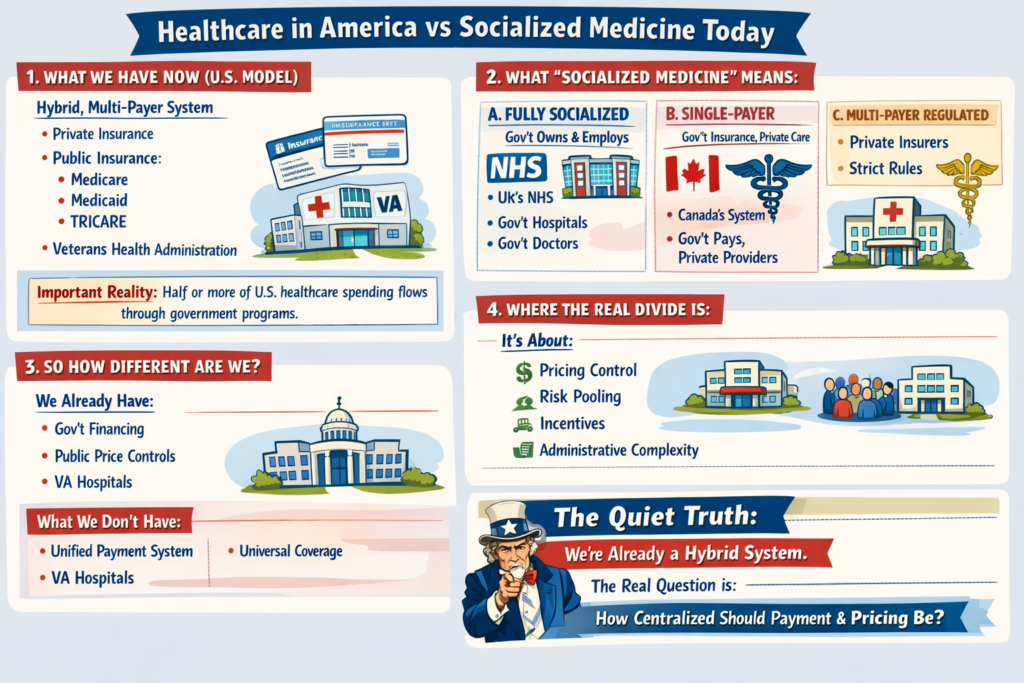
1. What We Have Now (U.S. Model)
The U.S. system is a hybrid, multi-payer system:
-
Private insurance (employer-based and individual market)
-
Public insurance:
-
Medicare
-
Medicaid
-
TRICARE
-
Veterans Health Administration
-
-
Private hospitals (mostly nonprofit, some for-profit)
-
Private physician practices (increasingly consolidated)
Important reality:
Roughly half or more of U.S. healthcare spending already flows through government programs. We are not a pure market system. We are a complex blend.
2. What “Socialized Medicine” Actually Means
People often use “socialized” loosely. There are actually three different models internationally:
A. Fully Socialized (Government Owns & Employs)
Example: National Health Service in the UK
-
Government owns hospitals
-
Doctors are government employees
-
Government sets budgets directly
-
Care funded through taxes
That’s true “socialized medicine.”
B. Single-Payer (Government Pays, Private Providers Deliver)
Example: Medicare (Canada’s system)
-
Private hospitals & doctors
-
Government is the main insurer
-
One public payment system
-
Funded via taxes
This is not government-run hospitals — it’s government-run insurance.
C. Multi-Payer Regulated System
Example: Statutory Health Insurance
-
Private and nonprofit insurers
-
Strict national rules
-
Price controls
-
Universal coverage mandate
3. So How Different Are We?
Structurally:
-
We already have heavy government financing.
-
We already regulate pricing in public programs.
-
We already operate large government-run care systems (VA hospitals).
-
We already subsidize private insurance through tax exclusions.
What we don’t have:
-
A unified payment structure
-
National price controls across the board
-
Universal automatic coverage
-
Simplified billing
The biggest structural difference isn’t just “who pays.”
It’s:
-
Fragmentation
-
Administrative layering
-
Pricing freedom in private markets
-
Employment-tied insurance
4. Where the Real Divide Is
The debate isn’t simply:
Private vs Socialized.
It’s about:
-
Who controls pricing?
-
How risk is pooled?
-
How incentives are aligned?
-
How much administrative complexity is tolerated?
Even a “socialized” system still rations care — just differently (wait times vs cost-sharing).
Even our current system has price controls — just unevenly applied.
5. If the U.S. “Moved Toward Socialized” — What Would Actually Change?
Not necessarily hospital ownership.
More likely changes would include:
-
Centralized bargaining power
-
Uniform reimbursement rates
-
Elimination of employer-based insurance
-
Tax-based funding instead of premium-based funding
-
Dramatically reduced administrative overhead
-
Reduced insurer role
The money flow changes.
The power centers shift.
Administrative structure simplifies.
But doctors would still practice medicine.
Hospitals would still exist.
Care would still be rationed — just through different mechanisms.
6. The Quiet Truth
We are already halfway between models.
The U.S. system is not a free market.
It is not socialized.
It is a layered hybrid with competing incentives.
The question isn’t:
“Would we become socialized?”
The real question is:
“How centralized do we want payment and pricing authority to be?”
That’s a structural debate — not just a funding debate.
To go deeper, we have to explore:
-
What would actually happen to costs?
-
What happens to innovation?
-
What happens to wait times?
-
Or what a realistic transition would look like?
The real questions aren’t ideological. They’re mechanical: