Healthcare in America, Follow the Money, Post 4 Following the Dollar
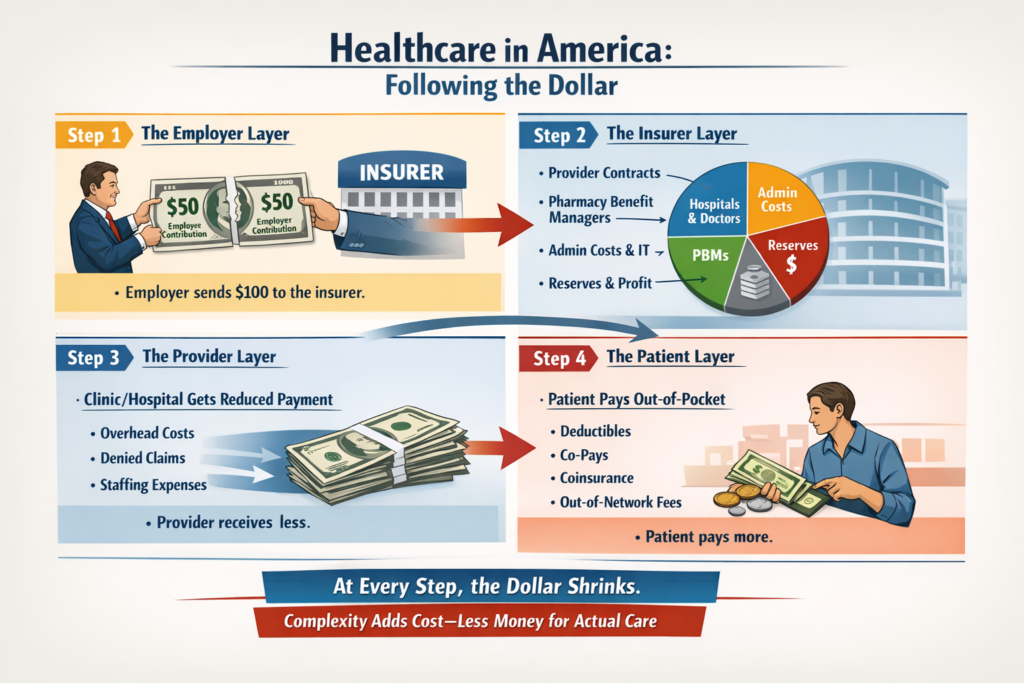
Step 1 — The Employer Layer
The $100 is collected as part of payroll. The employer passes it along to an insurer.
Even here, the dollar is split: part covers the premium contribution from the employee, part comes from the employer’s share. Often, employees never see this money — it’s folded into total compensation.
Step 2 — The Insurer Layer
The insurer receives the full $100. What happens next?
Provider network contracts: A portion is reserved to pay hospitals, clinics, and doctors who treat the plan’s members.
Pharmacy Benefit Managers (PBMs): Another slice goes to manage prescriptions, negotiate drug prices, and administer formularies.
Administrative costs: Claims processing, billing support, compliance, and IT systems take their share.
Reserves & profit: Insurers keep a portion in reserve or as profit.
At this stage, the dollar has already been carved up multiple times before it reaches clinical care.
Step 3 — The Provider Layer
When a patient visits a clinic or hospital, the dollar arrives in pieces.
The clinic receives its payment based on negotiated rates, not the sticker price.
Some funds are deducted for administrative overhead, billing, or staffing costs.
Denied claims or rejected charges may reduce the effective payment even further.
By the time the provider gets the money, a substantial portion has been diverted to administrative friction rather than patient care.
Step 4 — The Patient Layer
Even after this, the patient often pays out-of-pocket:
Deductibles
Co-pays
Coinsurance
Out-of-network charges
This means the same dollar has been contributed multiple times: first through the paycheck, then through taxes (if federal programs subsidize care), and again at the point of service.
Structural Insight
Following the dollar exposes a simple truth: complexity drives cost.
Each layer exists for a reason — regulation, risk management, negotiation, or compliance.
But layering creates inefficiency.
Patients, employers, and taxpayers see only fragments of the total flow.
And yet, the system appears opaque, expensive, and unpredictable — not because someone is “hiding” money, but because the machine is built to operate through multiple intermediaries.
Next Step:
Now that we’ve traced the dollar, we can examine administrative bloat and its effect on clinical care. This is where the incentives of the system meet reality, and where we start to see why costs escalate without necessarily improving outcomes.

 Healthcare in America, Follow the Money, Post 4 Following the Dollar
Healthcare in America, Follow the Money, Post 4 Following the Dollar