








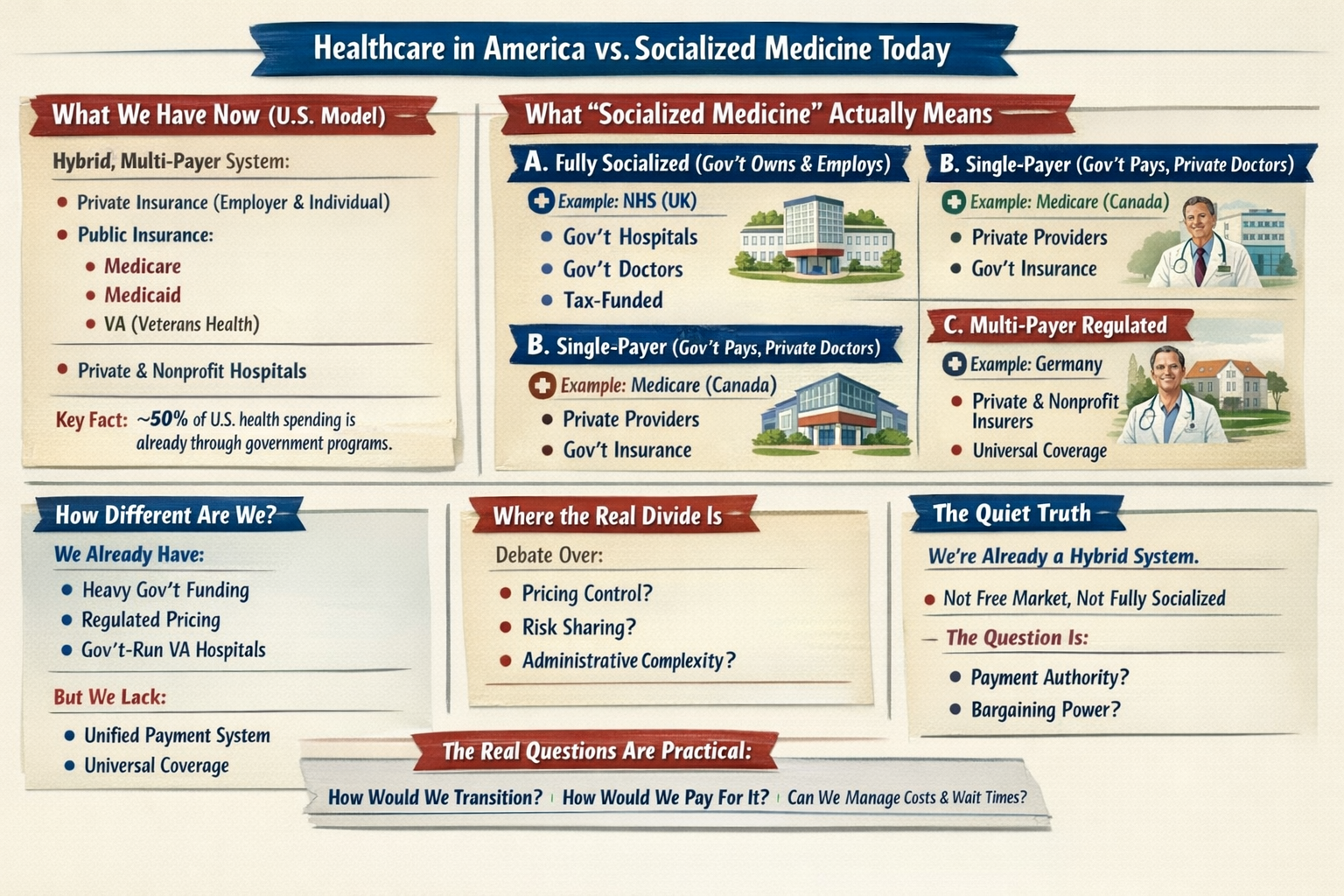
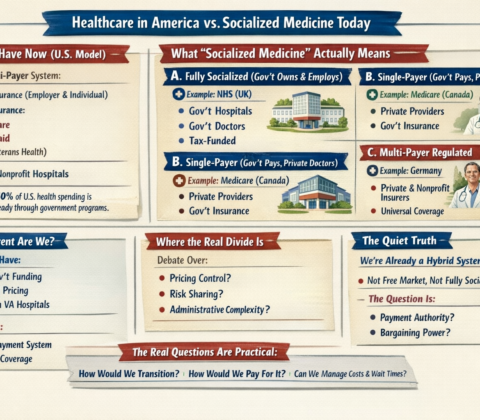
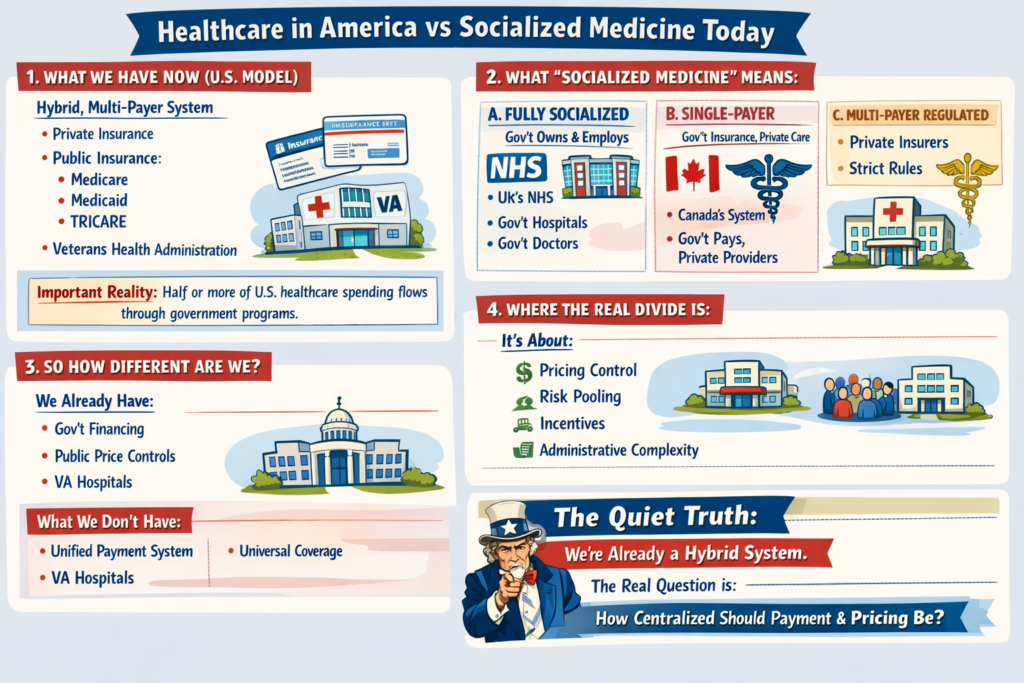
Healthcare in America vs Socialized Medicine Today
1. What We Have Now (U.S. Model)
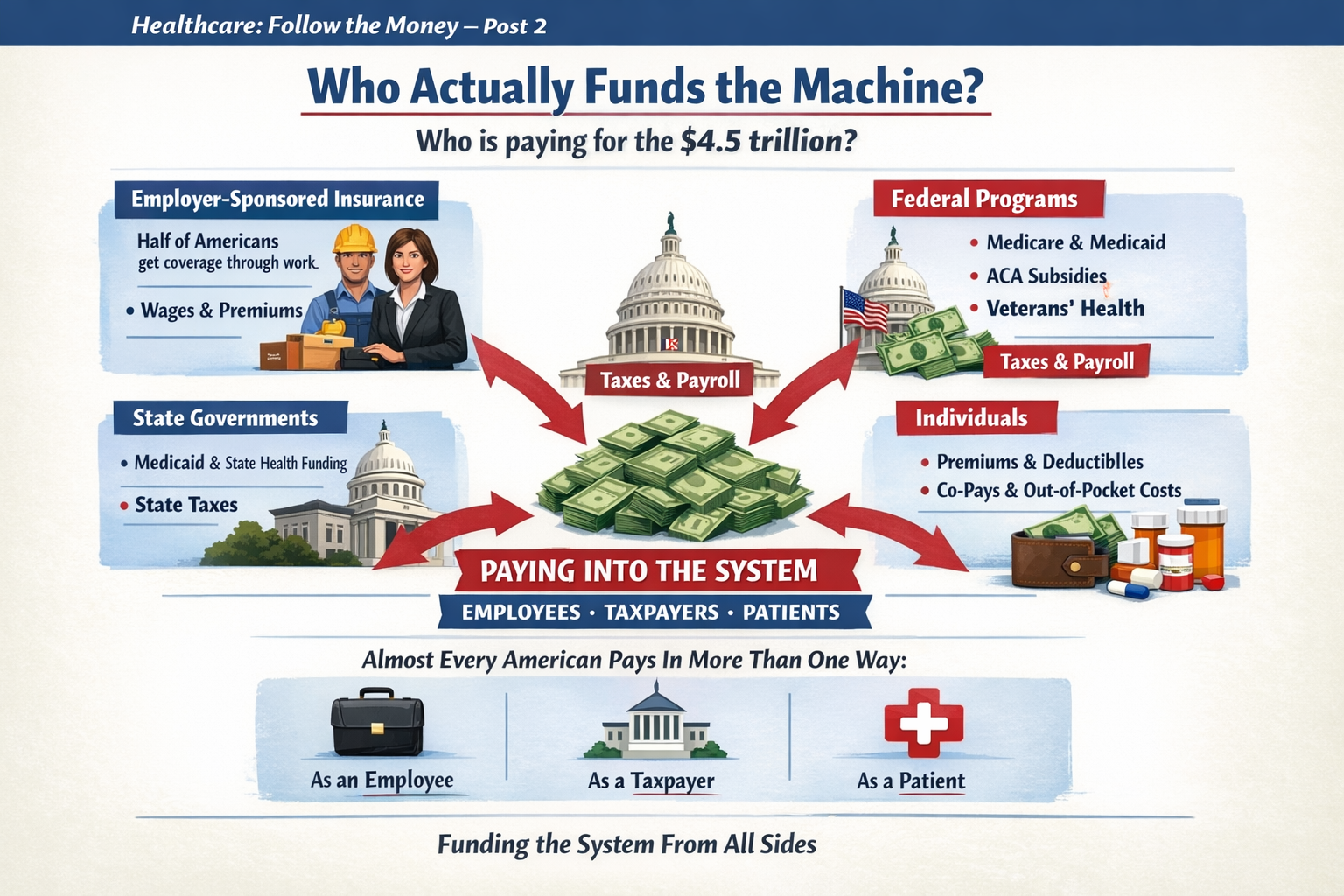
The U.S. system is a hybrid, multi-payer system:
-
Private insurance (employer-based and individual market)
-
Public insurance:
-
Medicare
-
Medicaid
-
TRICARE
-
Veterans Health Administration
-
-
Private hospitals (mostly nonprofit, some for-profit)
-
Private physician practices (increasingly consolidated)
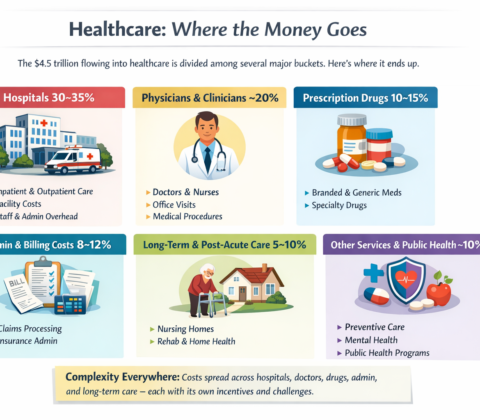
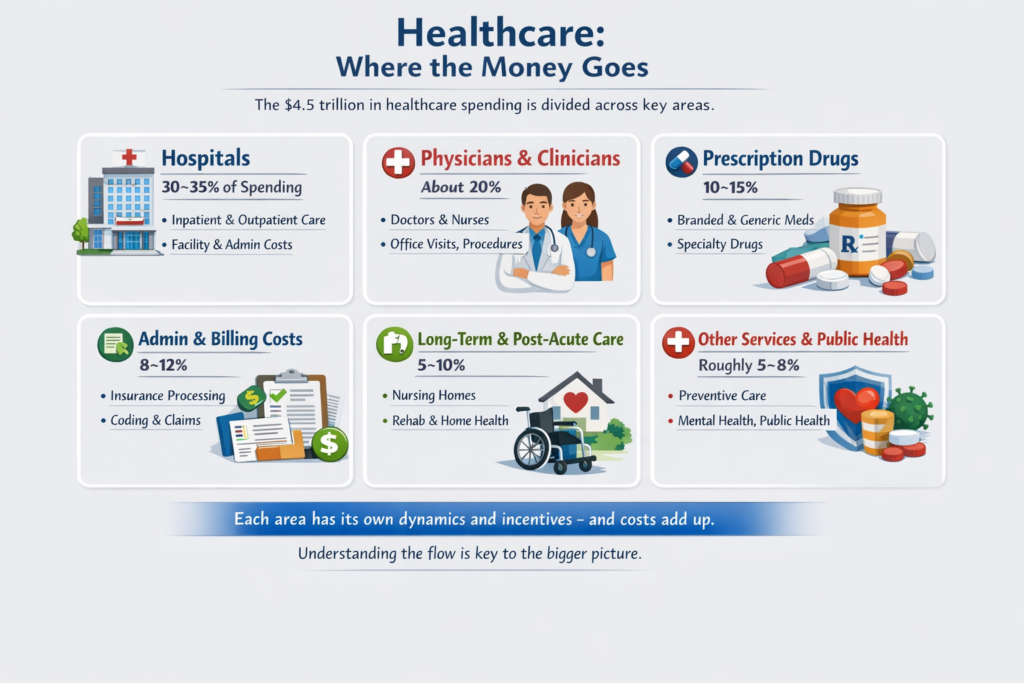
Important reality:
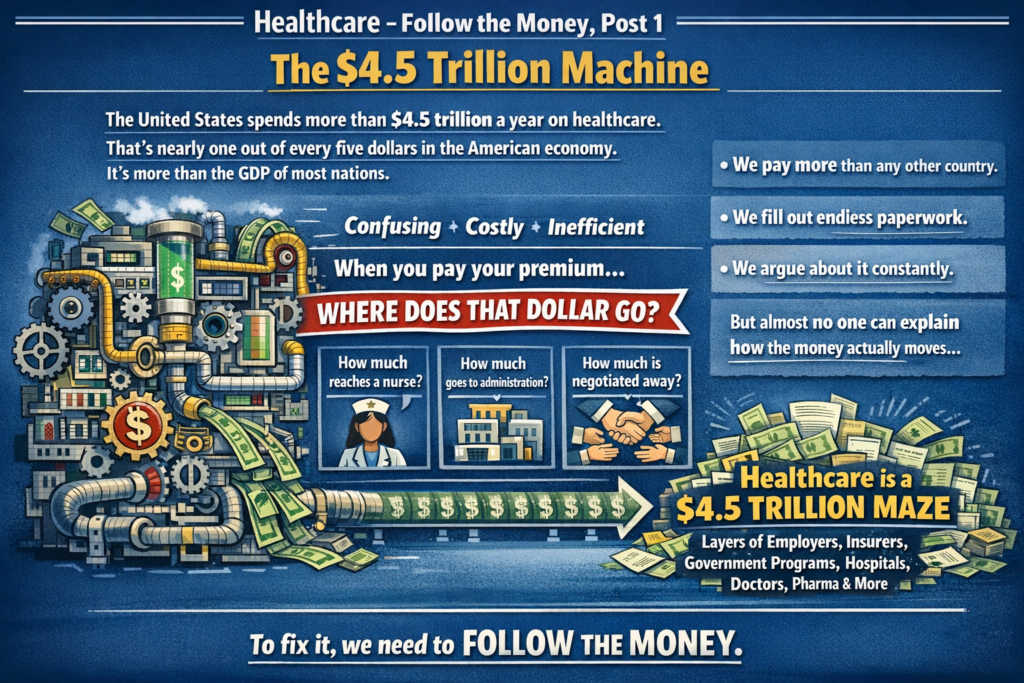
Roughly half or more of U.S. healthcare spending already flows through government programs. We are not a pure market system. We are a complex blend.
2. What “Socialized Medicine” Actually Means
People often use “socialized” loosely. There are actually three different models internationally:
A. Fully Socialized (Government Owns & Employs)
Example: National Health Service in the UK
-
Government owns hospitals
-
Doctors are government employees
-
Government sets budgets directly
-
Care funded through taxes
That’s true “socialized medicine.”
B. Single-Payer (Government Pays, Private Providers Deliver)
Example: Medicare (Canada’s system)
-
Private hospitals & doctors
-
Government is the main insurer
-
One public payment system
-
Funded via taxes
This is not government-run hospitals — it’s government-run insurance.
C. Multi-Payer Regulated System
Example: Statutory Health Insurance
-
Private and nonprofit insurers
-
Strict national rules
-
Price controls
-
Universal coverage mandate
3. So How Different Are We?
Structurally:
-
We already have heavy government financing.
-
We already regulate pricing in public programs.
-
We already operate large government-run care systems (VA hospitals).
-
We already subsidize private insurance through tax exclusions.
What we don’t have:
-
A unified payment structure
-
National price controls across the board
-
Universal automatic coverage
-
Simplified billing
The biggest structural difference isn’t just “who pays.”
It’s:
-
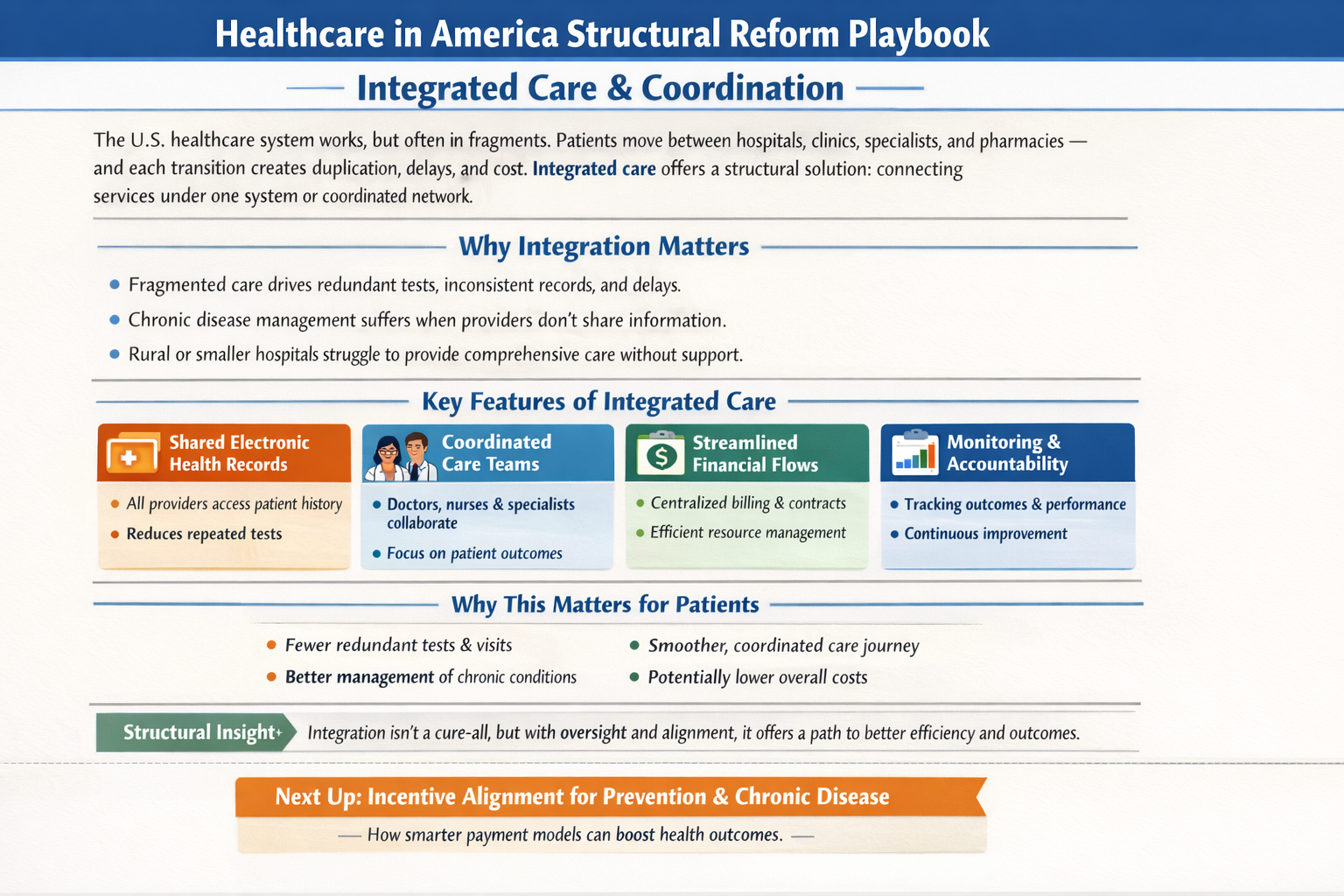
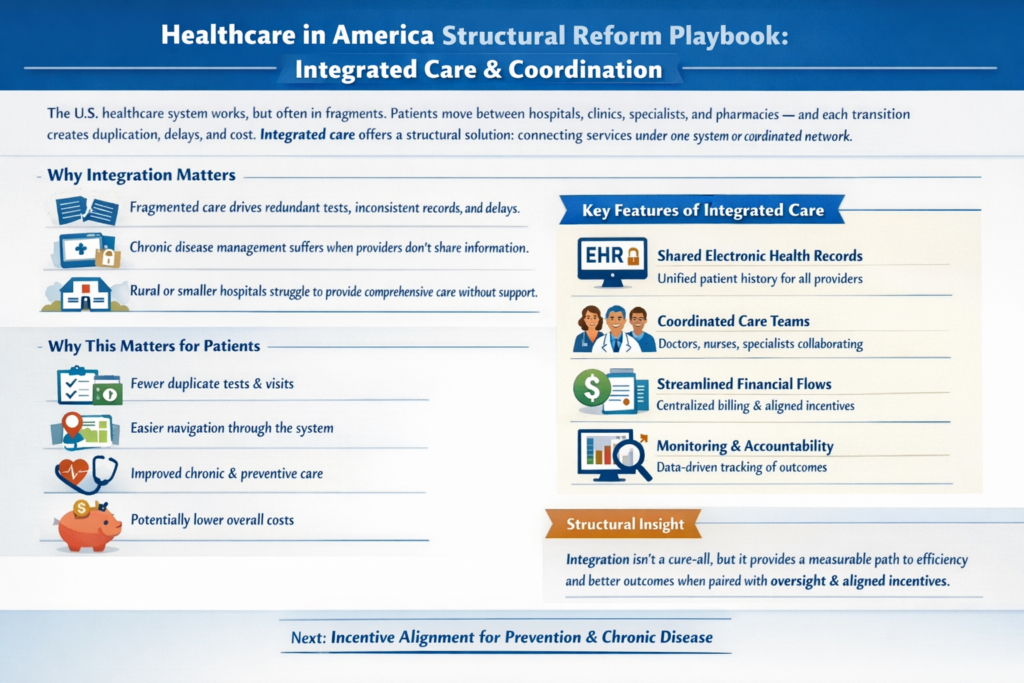
Fragmentation
-
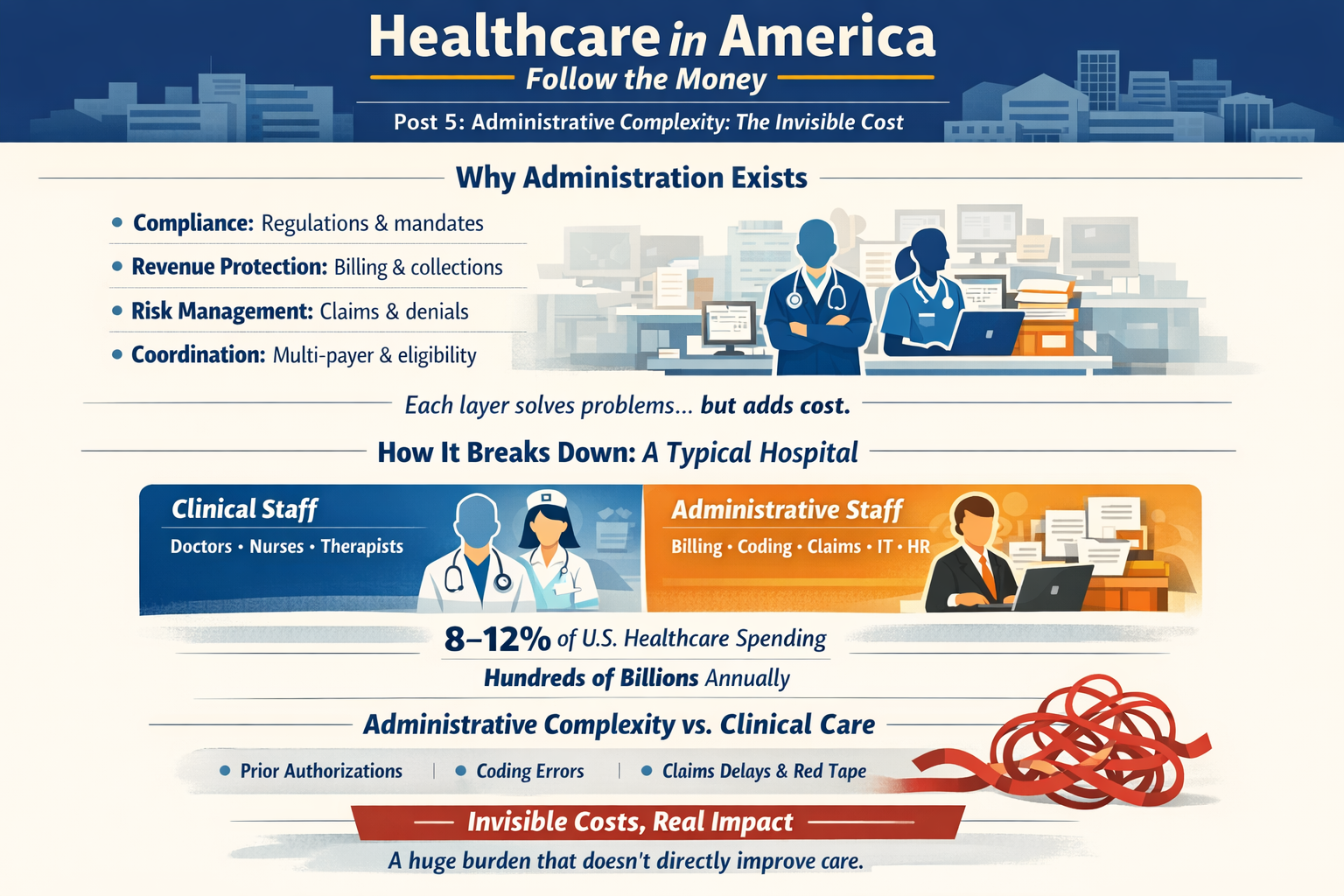
Administrative layering
-
Pricing freedom in private markets
-
Employment-tied insurance
4. Where the Real Divide Is
The debate isn’t simply:
Private vs Socialized.
It’s about:
-
Who controls pricing?
-
How risk is pooled?
-
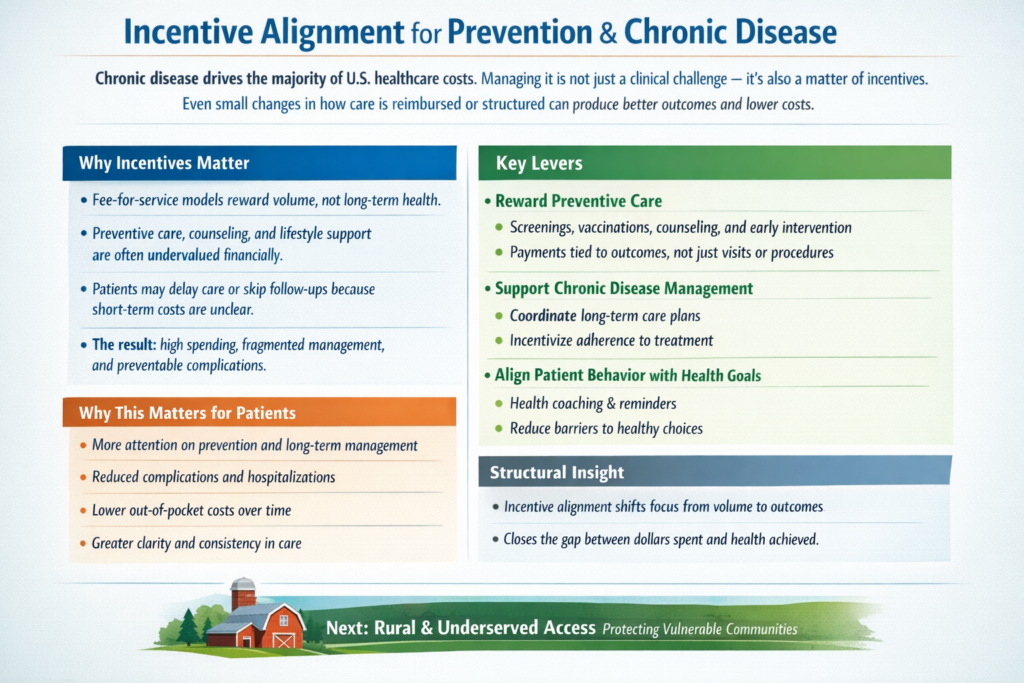
How incentives are aligned?
-
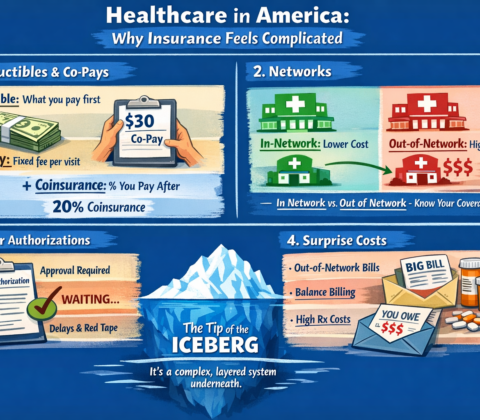
How much administrative complexity is tolerated?
Even a “socialized” system still rations care — just differently (wait times vs cost-sharing).
Even our current system has price controls — just unevenly applied.
5. If the U.S. “Moved Toward Socialized” — What Would Actually Change?
Not necessarily hospital ownership.
More likely changes would include:
-
Centralized bargaining power
-
Uniform reimbursement rates
-
Elimination of employer-based insurance
-
Tax-based funding instead of premium-based funding
-
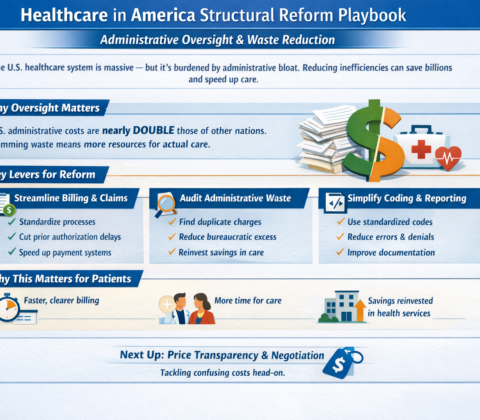
Dramatically reduced administrative overhead
-
Reduced insurer role
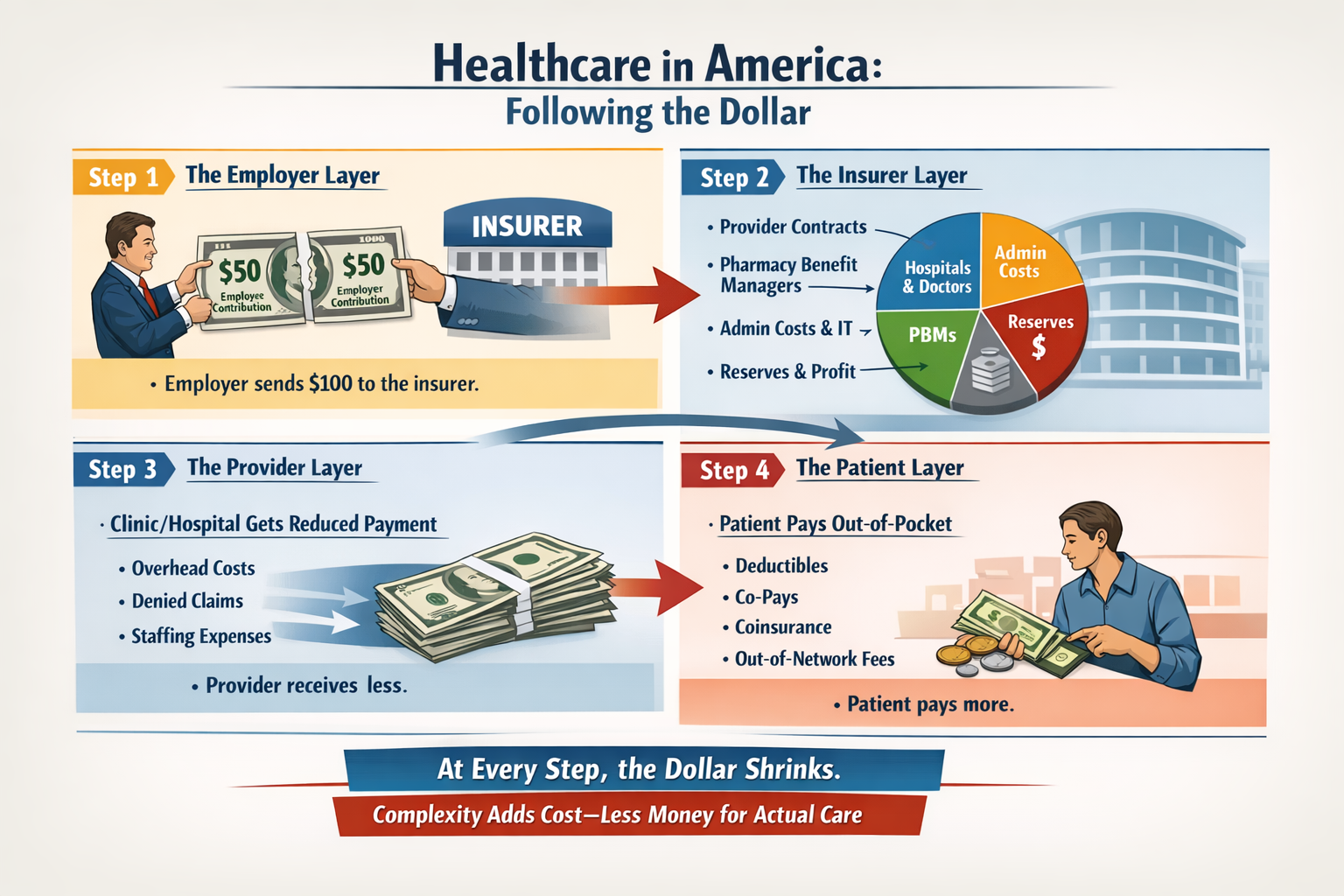
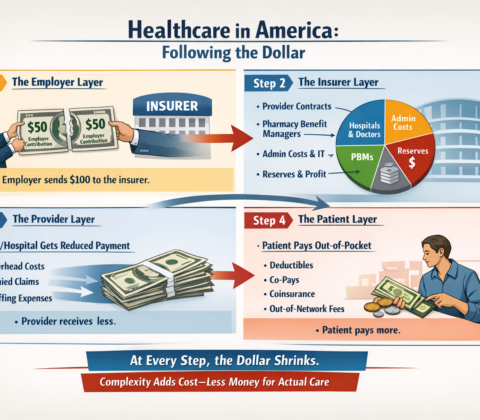
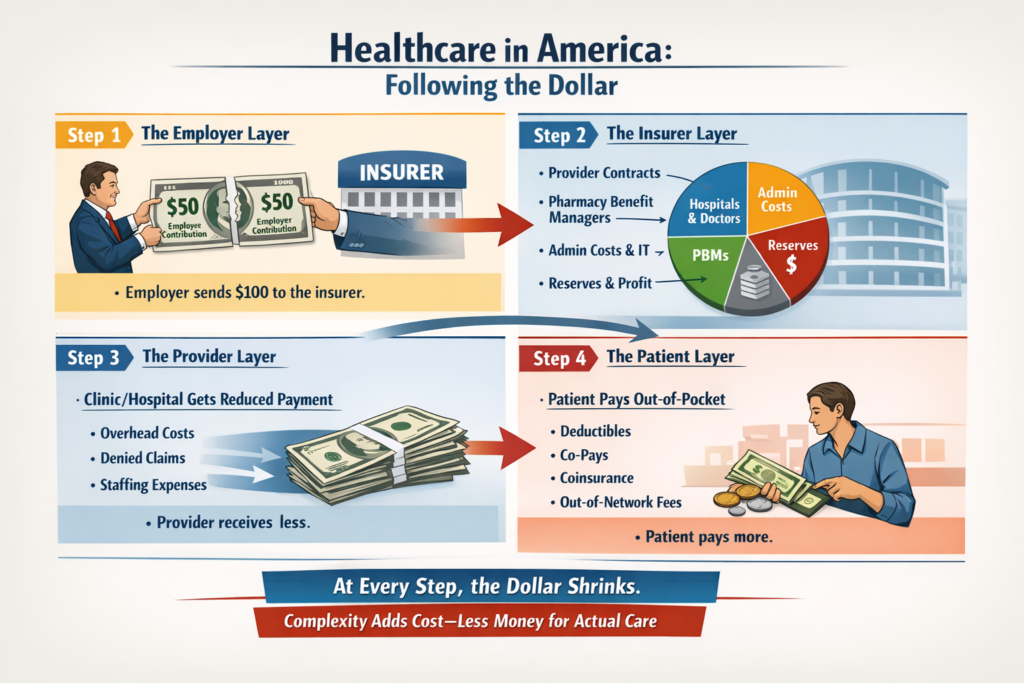
The money flow changes.
The power centers shift.
Administrative structure simplifies.
But doctors would still practice medicine.
Hospitals would still exist.
Care would still be rationed — just through different mechanisms.
6. The Quiet Truth
We are already halfway between models.
The U.S. system is not a free market.
It is not socialized.
It is a layered hybrid with competing incentives.
The question isn’t:
“Would we become socialized?”
The real question is:
“How centralized do we want payment and pricing authority to be?”
That’s a structural debate — not just a funding debate.
To go deeper, we have to explore:
-
What would actually happen to costs?
-
What happens to innovation?
-
What happens to wait times?
-
Or what a realistic transition would look like?
The real questions aren’t ideological. They’re mechanical:





























































































































 That’s right, saved 25% from last years meal. Only had to give up 50% of the food. Putz
That’s right, saved 25% from last years meal. Only had to give up 50% of the food. Putz

































































































































A Call to Action: Defund Corporate Media and Support Independent Voices
Public trust in mainstream media has collapsed — and for good reason. High-profile events like the Washington Post’s massive layoffs are not isolated incidents; they are symptoms of a deeper problem. Much of today’s media ecosystem is owned by billionaires, driven by shareholders, and shaped by advertising revenue and algorithmic incentives. Truth is no longer the priority. Profit is.
This isn’t accidental. Corporate news outlets — including social platforms that quietly manipulate what we see — are constrained by the same financial forces that keep them alive: advertisers, institutional investors, and elite ownership. Editorial independence becomes impossible when the bottom line comes first.
If we want real change, we need to respond in the only language that system understands: money.
Cancel subscriptions. Unsubscribe. Withdraw your support. Defund them.
Yes, that may mean giving up a favorite show or streaming service owned by a publicly traded media conglomerate — entities deeply entangled with institutional investors like Vanguard and BlackRock. So be it. Let them eat cake while we redirect our resources toward journalism that actually serves the public.
What to Support Instead
Rather than feeding corporate media, seek out independent creators — journalists and podcasters who prioritize truth over ideology and are funded directly by listeners, not advertisers or conglomerates.
Support voices across the political spectrum — left, right, and center — as long as they are genuinely independent and not beholden to corporate overlords. You don’t have to agree with everything they say. In fact, you probably shouldn’t. What matters is that you are allowed to hear it.
What mainstream media pushes today is often predetermined at levels far above our pay grades. The antidote is decentralization: many independent voices instead of a single manufactured narrative.
Below is a curated list of independent podcasts, grouped by general leaning for clarity. These recommendations are based on podcast directories, media reviews, and user feedback, and focus on shows that:
Are not owned by major media corporations
Emphasize factual reporting and honest analysis
Are funded primarily by listeners
Left-Leaning Independent Podcasts (Progressive, Anti-Corporate Focus)
These shows often critique corporate power, neoliberalism, and systemic inequality while remaining listener-supported.
Best of the Left
A long-running podcast curating progressive commentary on politics, culture, and economics. Produced by a small independent team, free of algorithmic manipulation or corporate backing. Funded through donations and memberships.
Rev Left Radio
An independently hosted show exploring leftist history, theory, and current events from a working-class perspective. Ad-free and supported by Patreon.
Secular Talk (Kyle Kulinski)
A fact-focused progressive commentary podcast emphasizing anti-establishment politics. Funded directly by viewers without corporate ownership.
The Humanist Report (Mike Figueredo)
Independent political commentary with a humanist and social justice lens. Fully listener-funded and unapologetically critical of media accountability failures.
Right-Leaning Independent Podcasts (Conservative, Free-Speech Focus)
These emphasize conservative values such as limited government and free expression while operating outside corporate media structures.
The Tucker Carlson Podcast
Independently produced following Carlson’s departure from Fox News. Features long-form interviews and commentary without network constraints, supported through subscriptions.
The Canadian Conservative
A solo-hosted, listener-supported podcast offering conservative commentary on Canadian and global political issues.
Relatable with Allie Beth Stuckey
An independent podcast blending conservative Christian perspectives with news analysis. Funded through ads and listener support, not corporate media ownership.
Centrist / Non-Partisan Independent Podcasts (Balanced, Media-Critical)
These shows aim to challenge narratives on both sides and prioritize context, evidence, and accountability.
On the Media
Produced by WNYC, a public radio outlet rather than a corporate media conglomerate. Focuses on media ethics, journalism practices, and narrative framing. Funded primarily by public donations.
The Purple Principle
An independent podcast seeking common ground by interviewing voices across the political spectrum. Fully listener-supported.
Left, Right & Center
A structured debate format featuring progressive, conservative, and moderate perspectives. Originally public radio, now widely distributed but still focused on civil, fact-based dialogue.
UNBIASED (Jordan Berman)
A daily, ad-free recap of U.S. news focused on facts rather than spin. Entirely listener-funded.
MeidasTouch Network
A lawyer-run independent media network offering fact-checked political analysis. Often left-leaning, but structured outside traditional corporate media.
Why This Matters
Independent journalism survives only if people are willing to support it directly. This shift isn’t easy — but it is powerful. Every canceled subscription and every dollar redirected helps weaken a system that no longer serves the public and strengthens one that still might.
If we want accountability, transparency, and honest debate, this is how we build it.
And yes — we could use a little help as well.
Share this:
Like this: