
Healthcare, how policies are developed and implemented.
On
- Menu
-
Who really makes the decisions (incentives, gatekeepers, power structures)
-
What access actually looks like on the ground
-
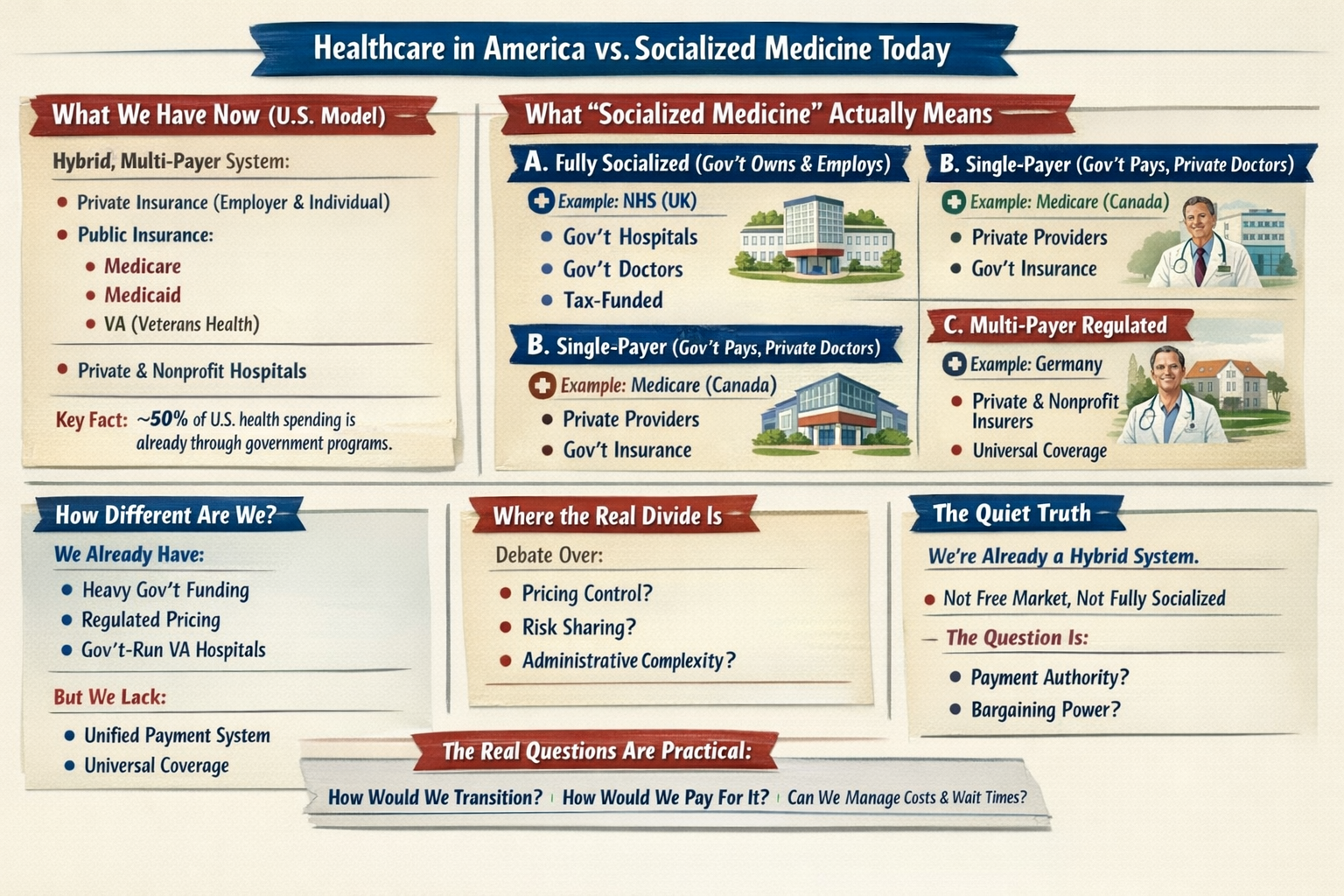
A clear comparison of free-market vs. socialized models — trade-offs, not team cheers
The goal isn’t to push an agenda; it’s to equip you with context so you can think, decide, and act from knowledge instead of reflexes.For the majority of my life, my knowledge of healthcare was condensed into these three or four questions, asked under stress:
-
Am I insured?
-
Will my spouse’s job still cover us?
-
What happens if we get pregnant / sick / laid off?
-
Can we afford this surprise?
Knowing the answers to those 4 questions is not enough.
Each section is intentionally concise: long enough to hold your attention, grounded enough to encourage independent research. By the end of the series, you’ll have a clearer, working understanding of healthcare and the government’s role in it—often more than many legislators themselves. More importantly, you’ll be able to see through political rhetoric and make informed judgments instead of relying on campaign slogans.
Thanks for reading along so far. If this resonates, stick around.
Just Published, working backwards |
In Order written and published |
|
|
|

















Comments are Disabled